Sebastiano Maria Colombo, Luigi Vivona, Michele Battistin, Vittorio Scaravilli, Alessandro Galli, Chiara Anzanello, Elisa Cipriani, Francesca Gori, Serena Todaro, Carlo Valsecchi, Daniele Dondossola, Anna Paola Marcello, Andrea Carlin, Antonio Pesenti, Giacomo Grasselli, Alberto Zanella
{"title":"Citrate regional anticoagulation of 500 ml/min of extracorporeal blood flow: an experimental study.","authors":"Sebastiano Maria Colombo, Luigi Vivona, Michele Battistin, Vittorio Scaravilli, Alessandro Galli, Chiara Anzanello, Elisa Cipriani, Francesca Gori, Serena Todaro, Carlo Valsecchi, Daniele Dondossola, Anna Paola Marcello, Andrea Carlin, Antonio Pesenti, Giacomo Grasselli, Alberto Zanella","doi":"10.1186/s40635-025-00771-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Regional citrate anticoagulation (RCA) is the most widespread technique which allows to perform extracorporeal treatments, avoiding the complications of systemic anticoagulation. Due to limited citrate clearance, RCA may be applied only to low extracorporeal blood flows (i.e., BF < 200 ml/min). In this proof of concept study, we developed an innovative RCA technique based on Ion Exchange Resin (i-ER) technology capable of regionally anticoagulating BF up to 500 mL/min.</p><p><strong>Methods: </strong>Six healthy swine (41.0 ± 3.1 kg) were sedated, mechanically ventilated, and connected to a prototype extracorporeal circuit for continuous renal replacement therapy featuring a citrate-removal stage based on absorbent materials and replacement fluids. Blood flow was 500 ml/min. Sodium citrate was continuously infused at the circuit inlet (5 mmol/L). Heparin was continuously infused. Citrate concentration and Kaolin Heparinase thromboelastography (KH-TEG) were measured on arterial blood, extracorporeal blood downstream the citrate infusion port, and downstream the citrate-removal stage. Samples were collected at baseline, 2, 8, 15, 30, 45, 60, 90, and 120 min for citrate and at baseline, 2, 30, 60, and 120 min for KH-TEG. Calcium chloride was infused to maintain systemic ionized calcium within the physiological range. The experiment lasted 2 h.</p><p><strong>Results: </strong>During the whole experiment, KH-TEG in the artery showed normal coagulation: reaction time (R) was 8.30[6.80-10.10] min, with Maximum Amplitude (MA) of 71.70[67.90-77.00] mm, while in the extracorporeal circuit, KH-TEG showed no sign of clot formation R > 60 min, MA = 0 mm. Citrate concentrations in blood samples were stable within 30 min, then slowly increased. The efficacy of the citrate-removal dropped from 93.8 ± 3.4% to 48.3 ± 1.5% at the beginning (2 min) and at the end (2 h), respectively (p < 0.001), due to loss of efficiency of the iERs.</p><p><strong>Conclusions: </strong>This study demonstrates that iER-based RCA is a feasible and effective technique for regional anticoagulation of extracorporeal blood flow up to 500 mL/min for 60 min without significant complications.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"64"},"PeriodicalIF":2.8000,"publicationDate":"2025-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12187626/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00771-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Regional citrate anticoagulation (RCA) is the most widespread technique which allows to perform extracorporeal treatments, avoiding the complications of systemic anticoagulation. Due to limited citrate clearance, RCA may be applied only to low extracorporeal blood flows (i.e., BF < 200 ml/min). In this proof of concept study, we developed an innovative RCA technique based on Ion Exchange Resin (i-ER) technology capable of regionally anticoagulating BF up to 500 mL/min.
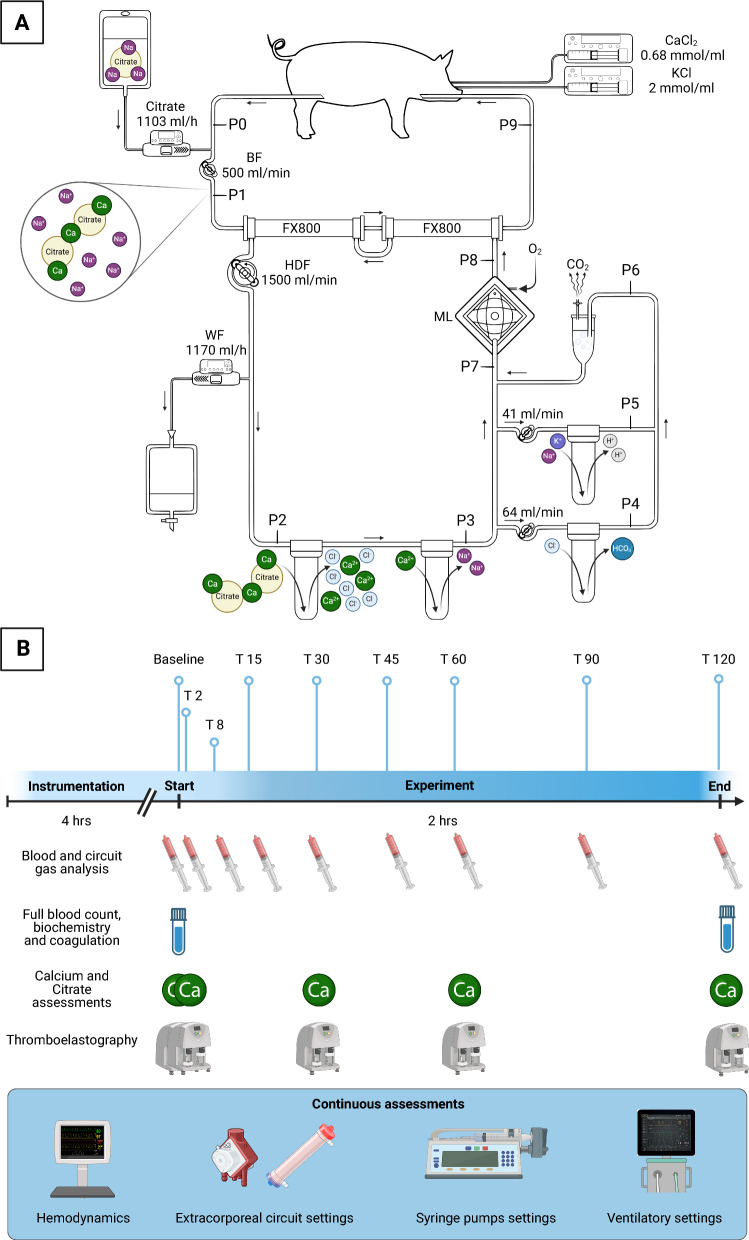
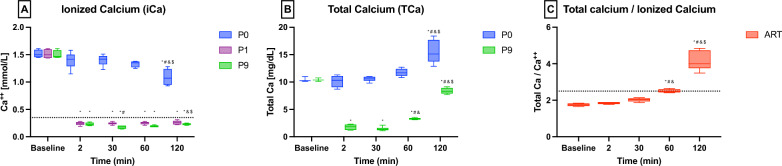
Methods: Six healthy swine (41.0 ± 3.1 kg) were sedated, mechanically ventilated, and connected to a prototype extracorporeal circuit for continuous renal replacement therapy featuring a citrate-removal stage based on absorbent materials and replacement fluids. Blood flow was 500 ml/min. Sodium citrate was continuously infused at the circuit inlet (5 mmol/L). Heparin was continuously infused. Citrate concentration and Kaolin Heparinase thromboelastography (KH-TEG) were measured on arterial blood, extracorporeal blood downstream the citrate infusion port, and downstream the citrate-removal stage. Samples were collected at baseline, 2, 8, 15, 30, 45, 60, 90, and 120 min for citrate and at baseline, 2, 30, 60, and 120 min for KH-TEG. Calcium chloride was infused to maintain systemic ionized calcium within the physiological range. The experiment lasted 2 h.
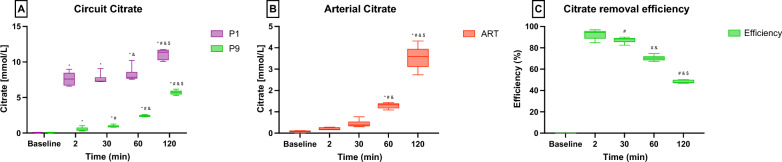
Results: During the whole experiment, KH-TEG in the artery showed normal coagulation: reaction time (R) was 8.30[6.80-10.10] min, with Maximum Amplitude (MA) of 71.70[67.90-77.00] mm, while in the extracorporeal circuit, KH-TEG showed no sign of clot formation R > 60 min, MA = 0 mm. Citrate concentrations in blood samples were stable within 30 min, then slowly increased. The efficacy of the citrate-removal dropped from 93.8 ± 3.4% to 48.3 ± 1.5% at the beginning (2 min) and at the end (2 h), respectively (p < 0.001), due to loss of efficiency of the iERs.
Conclusions: This study demonstrates that iER-based RCA is a feasible and effective technique for regional anticoagulation of extracorporeal blood flow up to 500 mL/min for 60 min without significant complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


