Gianpaolo Jannelli, Francesco Polinelli, Antonella Giardina, Marco Cuzzolin, Francesco Calvanese, Ivan Cabrilo, Luca Paun, Enrico Tessitore
{"title":"When can lumbar fusion be considered appropriate in the treatment of recurrent lumbar disc herniation? A systematic review and meta-analysis.","authors":"Gianpaolo Jannelli, Francesco Polinelli, Antonella Giardina, Marco Cuzzolin, Francesco Calvanese, Ivan Cabrilo, Luca Paun, Enrico Tessitore","doi":"10.1016/j.bas.2025.104285","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Recurrent lumbar disc herniation (RLDH) is defined as the reappearance, following initial discectomy, of disc material and pain after a period of at least six symptom-free months. Redo surgery is usually considered following unsuccessful conservative management or in the presence of neurological deficits.</p><p><strong>Research question: </strong>Given the lack of consensus on the ideal surgical strategy for RLDH, we conducted this study to evaluate when lumbar fusion (LF) should be considered in the treatment of RLDH.</p><p><strong>Material and methods: </strong>A literature search was conducted on PubMed, Google Scholar and clinicaltrials.gov focusing on the treatment of recurrent disc herniation using microdiscectomy alone or through fusion. The quality of the studies was evaluated using the Newcastle-Ottawa Quality Assessment Scale and Cochrane Risk of Bias Tool 2.0. The weighted mean difference was calculated for both binary and continuous outcomes.</p><p><strong>Results: </strong>This resulted in a list of 900 references, from which 11 studies were identified as meeting the inclusion criteria for the study. There were four prospective studies and seven retrospective studies. A comparison of LF and redo discectomy (RD) revealed no significant differences in clinical outcome scores. LF resulted in significantly higher intraoperative blood loss, longer hospitalizations and longer surgeries. No further differences were identified.</p><p><strong>Discussion and conclusions: </strong>Both LF and RD represent safe and effective treatment options in first RLDH. The choice of surgical strategy should integrate the eventual co-existence of clinical and radiological features of segmental instability, as well subjective aspects, such as surgeons' training and patient preference.</p>","PeriodicalId":72443,"journal":{"name":"Brain & spine","volume":"5 ","pages":"104285"},"PeriodicalIF":2.5000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12182769/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain & spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.bas.2025.104285","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Recurrent lumbar disc herniation (RLDH) is defined as the reappearance, following initial discectomy, of disc material and pain after a period of at least six symptom-free months. Redo surgery is usually considered following unsuccessful conservative management or in the presence of neurological deficits.
Research question: Given the lack of consensus on the ideal surgical strategy for RLDH, we conducted this study to evaluate when lumbar fusion (LF) should be considered in the treatment of RLDH.
Material and methods: A literature search was conducted on PubMed, Google Scholar and clinicaltrials.gov focusing on the treatment of recurrent disc herniation using microdiscectomy alone or through fusion. The quality of the studies was evaluated using the Newcastle-Ottawa Quality Assessment Scale and Cochrane Risk of Bias Tool 2.0. The weighted mean difference was calculated for both binary and continuous outcomes.
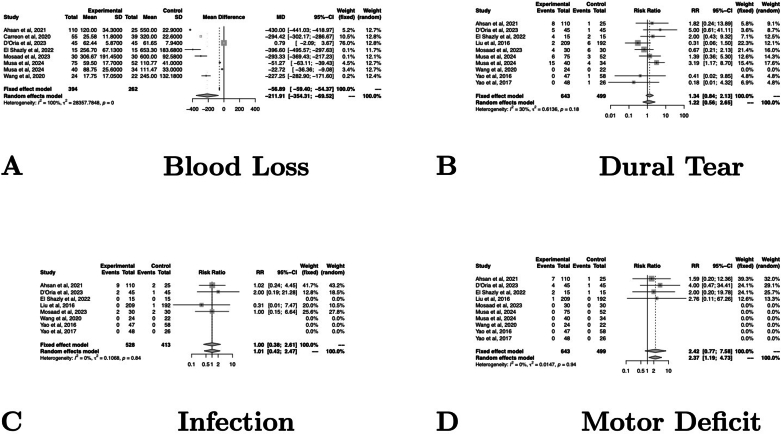
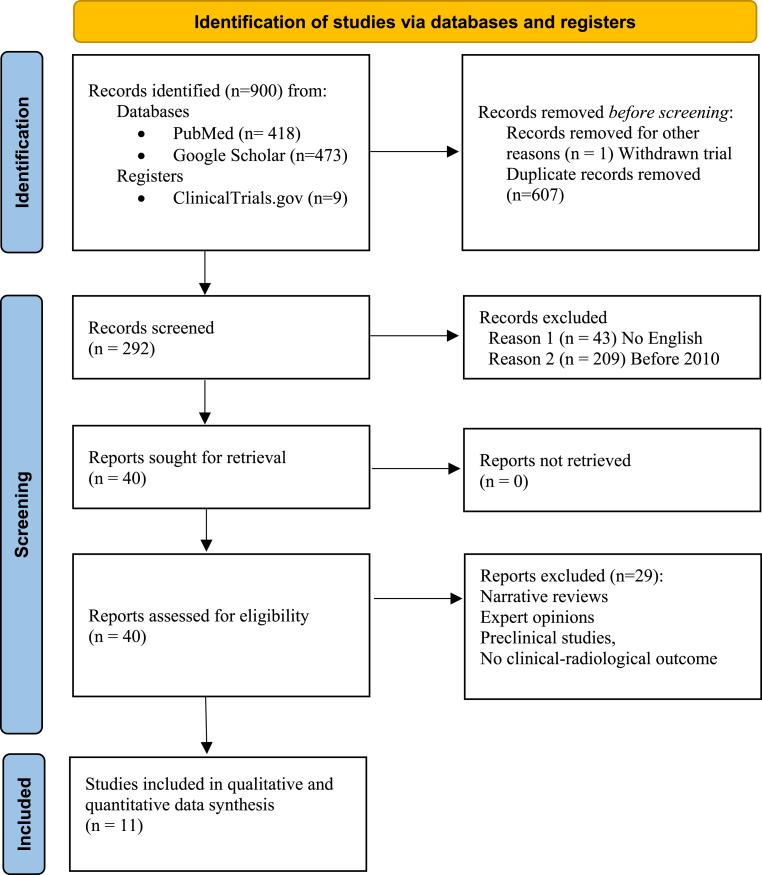
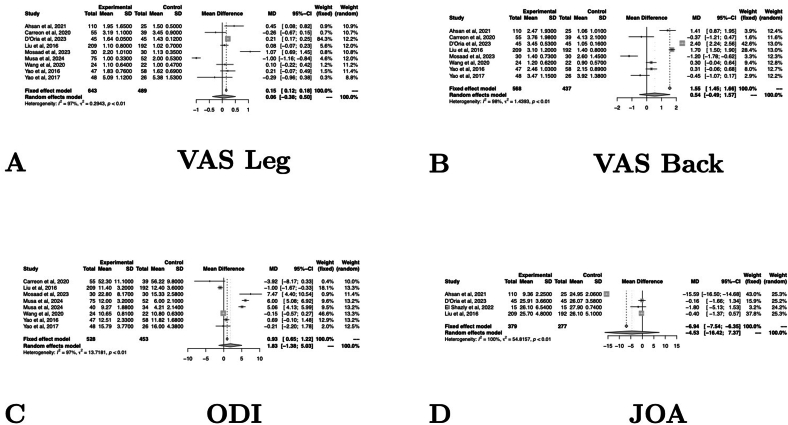
Results: This resulted in a list of 900 references, from which 11 studies were identified as meeting the inclusion criteria for the study. There were four prospective studies and seven retrospective studies. A comparison of LF and redo discectomy (RD) revealed no significant differences in clinical outcome scores. LF resulted in significantly higher intraoperative blood loss, longer hospitalizations and longer surgeries. No further differences were identified.
Discussion and conclusions: Both LF and RD represent safe and effective treatment options in first RLDH. The choice of surgical strategy should integrate the eventual co-existence of clinical and radiological features of segmental instability, as well subjective aspects, such as surgeons' training and patient preference.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


