{"title":"Adverse birth outcomes and associated factors among Sub-Saharan African grand multiparas: a systematic review and meta-analysis.","authors":"Agerie Mengistie Zeleke, Getnet Azanaw Takele, Yosef Aragaw Gonete, Yeshiwas Ayale Ferede, Worku Chekol Tassew","doi":"10.1177/26334941251342121","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adverse birth outcomes associated with grand multiparity are more ambiguous than those linked to multiparity. The primary literature on this issue reveals inconsistent findings across various studies. A paucity of data is evident in systematic reviews and meta-analyses that assess adverse birth outcomes specifically for African grand multiparas.</p><p><strong>Objectives: </strong>To address the pooled adverse birth outcomes and their associated factors among African grand multiparas.</p><p><strong>Design: </strong>Systematic review and meta-analysis.</p><p><strong>Data sources and methods: </strong>Studies were systematically searched from April 20, 2024, to June 15, 2024, using Scopus, Web of Science, PubMed, Science Direct, African Journal Online, and the Wiley Online Library. The Joanna Briggs Institute tool was used for a quality assessment of each primary study. Data were extracted using Excel and analyzed with Stata 11 software. A random-effects model was employed to calculate the pooled estimates. The paper employs appropriate statistical techniques to assess publication bias and heterogeneity, such as the symmetry of the funnel plot, Egger's test, and Cochran's <i>Q</i> test. The study addresses a critical public health issue in Africa, contributing valuable data that could inform policy and healthcare practices aimed at reducing adverse birth outcomes among grand multiparas. A subgroup analysis was performed based on the publication years.</p><p><strong>Results: </strong>The pooled prevalence of adverse birth outcomes among African grand multiparas was 24.97%; 95% CI: 19.97-31.99. Pregnancy-related complications (AOR: 3.17; 95% CI: 2.35-4.28), a history of home births (AOR: 3.30; 95% CI: 1.70-6.40), and rural residence (AOR: 4.12; 95% CI: 3.12-5.44) were significantly associated with adverse birth outcomes among African grand multiparas.</p><p><strong>Conclusion: </strong>Overall, the pooled prevalence of adverse birth outcomes among grand multiparas was comparably high. Variables such as rural residence, previous pregnancy-related complications, and a history of home births were significantly associated with adverse birth outcomes. Strengthening institutional births, providing high-quality prenatal care, and early pregnancy follow-ups are recommended to reduce adverse birth outcomes in grand multiparous women. In addition, improving the availability of comprehensive contraceptive options for rural-residing African grand multiparous women is essential.</p><p><strong>Prospero registration: </strong>CRD42024569768.</p>","PeriodicalId":75219,"journal":{"name":"Therapeutic advances in reproductive health","volume":"19 ","pages":"26334941251342121"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12181738/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic advances in reproductive health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334941251342121","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adverse birth outcomes associated with grand multiparity are more ambiguous than those linked to multiparity. The primary literature on this issue reveals inconsistent findings across various studies. A paucity of data is evident in systematic reviews and meta-analyses that assess adverse birth outcomes specifically for African grand multiparas.
Objectives: To address the pooled adverse birth outcomes and their associated factors among African grand multiparas.
Design: Systematic review and meta-analysis.
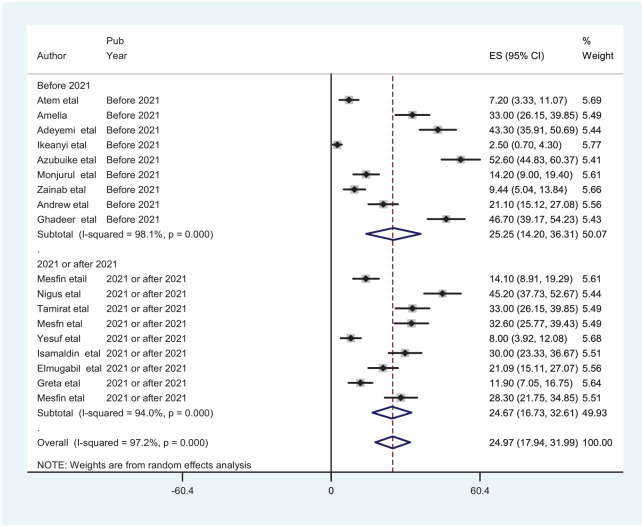
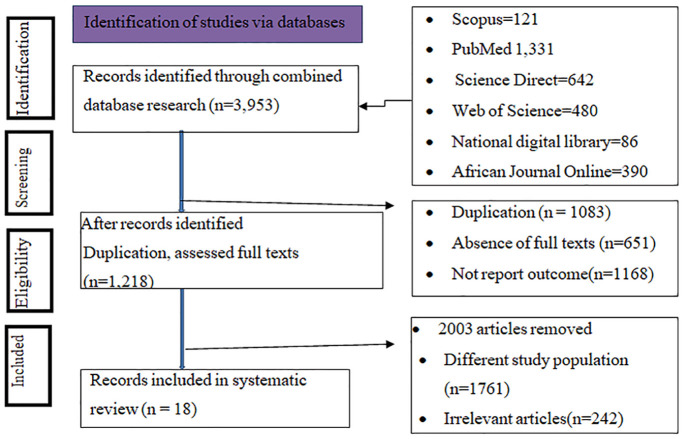
Data sources and methods: Studies were systematically searched from April 20, 2024, to June 15, 2024, using Scopus, Web of Science, PubMed, Science Direct, African Journal Online, and the Wiley Online Library. The Joanna Briggs Institute tool was used for a quality assessment of each primary study. Data were extracted using Excel and analyzed with Stata 11 software. A random-effects model was employed to calculate the pooled estimates. The paper employs appropriate statistical techniques to assess publication bias and heterogeneity, such as the symmetry of the funnel plot, Egger's test, and Cochran's Q test. The study addresses a critical public health issue in Africa, contributing valuable data that could inform policy and healthcare practices aimed at reducing adverse birth outcomes among grand multiparas. A subgroup analysis was performed based on the publication years.
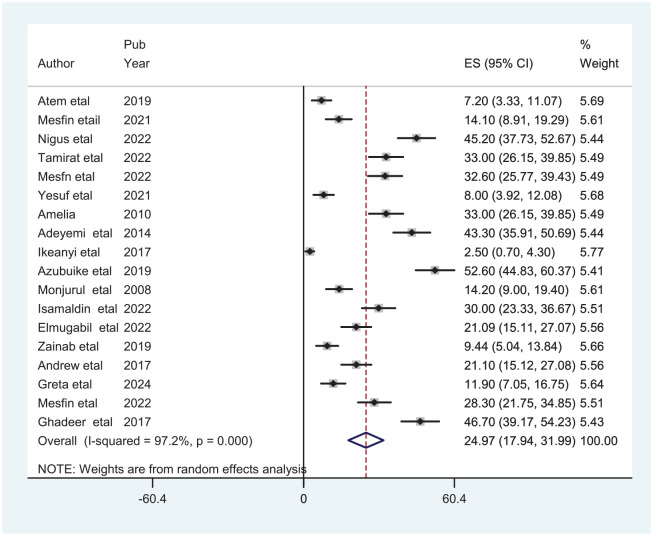
Results: The pooled prevalence of adverse birth outcomes among African grand multiparas was 24.97%; 95% CI: 19.97-31.99. Pregnancy-related complications (AOR: 3.17; 95% CI: 2.35-4.28), a history of home births (AOR: 3.30; 95% CI: 1.70-6.40), and rural residence (AOR: 4.12; 95% CI: 3.12-5.44) were significantly associated with adverse birth outcomes among African grand multiparas.
Conclusion: Overall, the pooled prevalence of adverse birth outcomes among grand multiparas was comparably high. Variables such as rural residence, previous pregnancy-related complications, and a history of home births were significantly associated with adverse birth outcomes. Strengthening institutional births, providing high-quality prenatal care, and early pregnancy follow-ups are recommended to reduce adverse birth outcomes in grand multiparous women. In addition, improving the availability of comprehensive contraceptive options for rural-residing African grand multiparous women is essential.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


