{"title":"Economic evaluation of inpatient medication reconciliation with a subtraction strategy.","authors":"Nontakorn Khomsanoi, Theetad Chombandit, Jurinporn Wiwatmanaskul, Chatchai Kreepala","doi":"10.1186/s13561-025-00649-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>University-based hospitals in Thailand face increasing financial strain due to insufficient reimbursement for inpatient care. The public health financing system comprises three major schemes: the Universal Coverage Scheme (UCS), Social Security Scheme (SSS), and Civil Servant Medical Benefit Scheme (CSMBS), which differ in funding mechanisms and reimbursement rates. Although all schemes apply the Diagnosis-Related Groups (DRG) system for inpatient payment, variations in base rates and case-mix complexity often leave tertiary hospitals underfunded. Medication reconciliation (MR) with a subtraction strategy-deducting patients' home medications from discharge prescriptions-has been implemented to optimize hospital resources. This study aimed to evaluate cost savings and identify key determinants influencing the economic outcomes of MR across public insurance schemes.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of 563 hospitalized internal medicine patients at a university-based hospital. Of these, 324 underwent MR with subtraction. Cost savings and reimbursement margins were calculated from the provider's perspective. Patients were stratified by healthcare scheme (CSMBS, UCS, SSS) and length of stay (LOS). Generalized Linear Mixed Models were used to identify factors associated with cost savings.</p><p><strong>Results: </strong>The highest mean cost savings per patient were observed in the SSS group (508.5 ± 56.1 THB [~ 14.1 USD]), and the lowest in CSMBS (133.5 ± 23.6 THB [~ 3.7 USD]). Prolonged LOS was associated with significantly greater savings (LOS > 21 days: IRR = 2.45, p < 0.001). SSS patients achieved the greatest overall savings (IRR = 3.95, p < 0.001). Nonetheless, negative reimbursement margins persisted across all schemes.</p><p><strong>Conclusions: </strong>Although MR with subtraction achieved measurable cost savings, it failed to offset reimbursement deficits. Broader financial reforms are needed to ensure sustainability, with MR positioned as a potentially scalable strategy within value-based care frameworks.</p>","PeriodicalId":46936,"journal":{"name":"Health Economics Review","volume":"15 1","pages":"52"},"PeriodicalIF":3.3000,"publicationDate":"2025-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12181825/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Economics Review","FirstCategoryId":"96","ListUrlMain":"https://doi.org/10.1186/s13561-025-00649-0","RegionNum":3,"RegionCategory":"经济学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: University-based hospitals in Thailand face increasing financial strain due to insufficient reimbursement for inpatient care. The public health financing system comprises three major schemes: the Universal Coverage Scheme (UCS), Social Security Scheme (SSS), and Civil Servant Medical Benefit Scheme (CSMBS), which differ in funding mechanisms and reimbursement rates. Although all schemes apply the Diagnosis-Related Groups (DRG) system for inpatient payment, variations in base rates and case-mix complexity often leave tertiary hospitals underfunded. Medication reconciliation (MR) with a subtraction strategy-deducting patients' home medications from discharge prescriptions-has been implemented to optimize hospital resources. This study aimed to evaluate cost savings and identify key determinants influencing the economic outcomes of MR across public insurance schemes.
Methods: We conducted a retrospective cohort study of 563 hospitalized internal medicine patients at a university-based hospital. Of these, 324 underwent MR with subtraction. Cost savings and reimbursement margins were calculated from the provider's perspective. Patients were stratified by healthcare scheme (CSMBS, UCS, SSS) and length of stay (LOS). Generalized Linear Mixed Models were used to identify factors associated with cost savings.
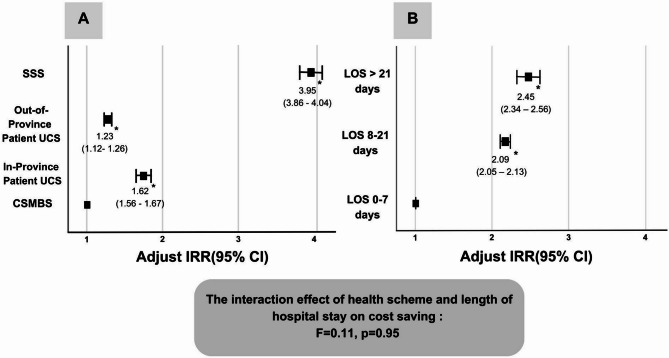
Results: The highest mean cost savings per patient were observed in the SSS group (508.5 ± 56.1 THB [~ 14.1 USD]), and the lowest in CSMBS (133.5 ± 23.6 THB [~ 3.7 USD]). Prolonged LOS was associated with significantly greater savings (LOS > 21 days: IRR = 2.45, p < 0.001). SSS patients achieved the greatest overall savings (IRR = 3.95, p < 0.001). Nonetheless, negative reimbursement margins persisted across all schemes.
Conclusions: Although MR with subtraction achieved measurable cost savings, it failed to offset reimbursement deficits. Broader financial reforms are needed to ensure sustainability, with MR positioned as a potentially scalable strategy within value-based care frameworks.
期刊介绍:
Health Economics Review is an international high-quality journal covering all fields of Health Economics. A broad range of theoretical contributions, empirical studies and analyses of health policy with a health economic focus will be considered for publication. Its scope includes macro- and microeconomics of health care financing, health insurance and reimbursement as well as health economic evaluation, health services research and health policy analysis. Further research topics are the individual and institutional aspects of health care management and the growing importance of health care in developing countries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


