Anton Alexander Nolte Peterlin, Louise Kruse Jensen, Emil Gleipner-Andersen, Hans Gottlieb
{"title":"CLOSE-UP - a favourable protocol for limb-sparing surgery of diabetic foot osteomyelitis.","authors":"Anton Alexander Nolte Peterlin, Louise Kruse Jensen, Emil Gleipner-Andersen, Hans Gottlieb","doi":"10.5194/jbji-10-199-2025","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b>: Diabetic foot osteomyelitis (DFO) is a severe complication of diabetic foot ulcers, leading to high morbidity, mortality, and major limb amputation risk. While limb-sparing surgery is well established, optimal wound closure and intraosseous antibiotic strategies remain under-explored and under-reported. This study evaluates a single-stage limb-sparing surgical approach incorporating primary closure and local intraosseous antibiotic therapy. <b>Methods</b>: This retrospective study included 97 DFO patients (2017-2024) treated using the CLOSE-UP (Conservative surgery, Local antibiotics, Oral versus intravenous antibiotics - OVIVA, Samples, Effective limb preservation, and closUre Primary) protocol, developed to standardize DFO surgery. The one-stage procedure involved bone sampling, local debridement or minor amputation (distal to the tarsometatarsal joint), antibiotic-loaded calcium sulfate-hydroxyapatite biocomposite application, and primary wound closure. Postoperatively, patients followed the OVIVA antimicrobial protocol: 1 week of intravenous (IV) therapy and 5 weeks of oral (empiric penicillin-cloxacillin) therapy. The primary outcome was treatment failure within 1 year, with a minimum follow-up of 12 months. <b>Results</b>: Clinical failure occurred in 13 patients (13.4 %), with only 4 patients (4.1 %) requiring major amputation. Peripheral arterial disease was present in 24 patients (24.7 %) and was the only variable significantly associated with clinical failure (odds ratios: 10.21; <math><mrow><mi>P</mi> <mo><</mo> <mn>0.01</mn></mrow> </math> ). The 1-year and 3-year mortality rates were 14.4 % and 35.9 %, respectively. <b>Conclusions</b>: The CLOSE-UP protocol demonstrated favourable outcomes. Given the high risk of mortality and limb loss in DFO, this structured approach has the potential to improve mobility, shorten rehabilitation, lower costs, and enhance quality of life. Further research, particularly randomized controlled trials, should focus on optimizing wound closure to improve long-term limb preservation and survival.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"10 3","pages":"199-206"},"PeriodicalIF":2.8000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12177510/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-10-199-2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
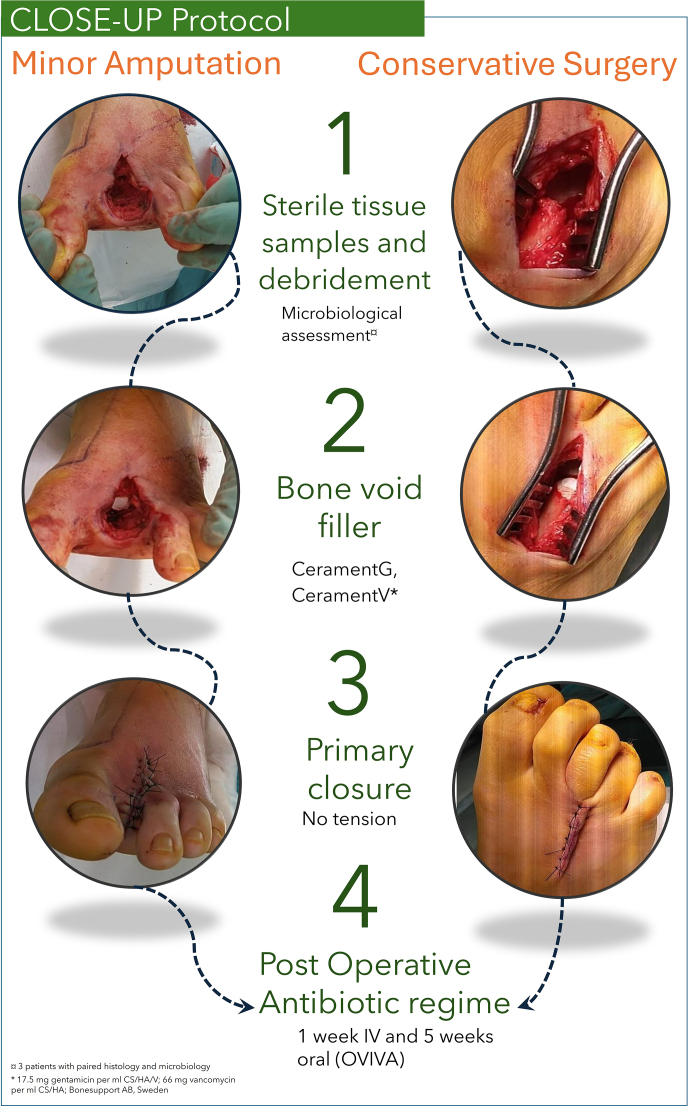
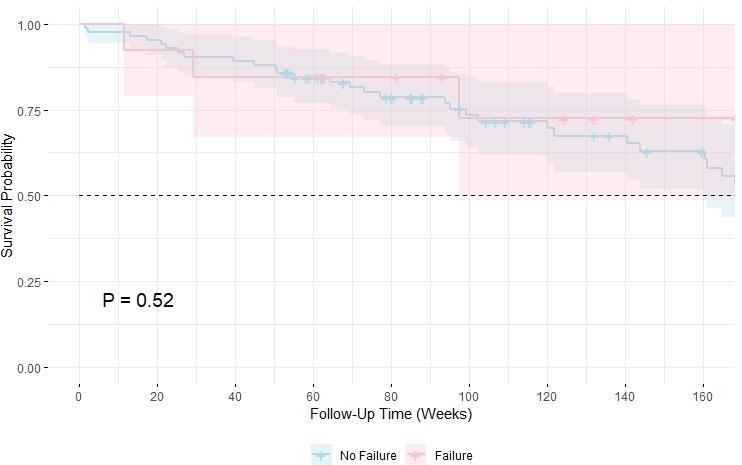
Introduction: Diabetic foot osteomyelitis (DFO) is a severe complication of diabetic foot ulcers, leading to high morbidity, mortality, and major limb amputation risk. While limb-sparing surgery is well established, optimal wound closure and intraosseous antibiotic strategies remain under-explored and under-reported. This study evaluates a single-stage limb-sparing surgical approach incorporating primary closure and local intraosseous antibiotic therapy. Methods: This retrospective study included 97 DFO patients (2017-2024) treated using the CLOSE-UP (Conservative surgery, Local antibiotics, Oral versus intravenous antibiotics - OVIVA, Samples, Effective limb preservation, and closUre Primary) protocol, developed to standardize DFO surgery. The one-stage procedure involved bone sampling, local debridement or minor amputation (distal to the tarsometatarsal joint), antibiotic-loaded calcium sulfate-hydroxyapatite biocomposite application, and primary wound closure. Postoperatively, patients followed the OVIVA antimicrobial protocol: 1 week of intravenous (IV) therapy and 5 weeks of oral (empiric penicillin-cloxacillin) therapy. The primary outcome was treatment failure within 1 year, with a minimum follow-up of 12 months. Results: Clinical failure occurred in 13 patients (13.4 %), with only 4 patients (4.1 %) requiring major amputation. Peripheral arterial disease was present in 24 patients (24.7 %) and was the only variable significantly associated with clinical failure (odds ratios: 10.21; ). The 1-year and 3-year mortality rates were 14.4 % and 35.9 %, respectively. Conclusions: The CLOSE-UP protocol demonstrated favourable outcomes. Given the high risk of mortality and limb loss in DFO, this structured approach has the potential to improve mobility, shorten rehabilitation, lower costs, and enhance quality of life. Further research, particularly randomized controlled trials, should focus on optimizing wound closure to improve long-term limb preservation and survival.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


