Hye Sung Kim, Wongi Woo, Young-Geun Choi, Ankit Bharat, Young Kwang Chae
{"title":"Novel association between graft rejection and post-transplant malignancy in solid organ transplantation.","authors":"Hye Sung Kim, Wongi Woo, Young-Geun Choi, Ankit Bharat, Young Kwang Chae","doi":"10.5500/wjt.v15.i2.102384","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Advancements in immunosuppressive therapies have improved graft survival by enhancing graft tolerance and preventing organ rejection. However, the risk of malignancy associated with prolonged immunosuppression remains a concern, as it can adversely affect recipients' quality of life and survival. While the link between immunosuppression and increased cancer risk is well-documented, the specific interactions between graft rejection and post-transplant malignancy (PTM) remain poorly understood. Addressing this knowledge gap is crucial for devising immunosuppressive strategies that balance rejection prevention with cancer risk reduction.</p><p><strong>Aim: </strong>To investigate whether immunosuppression in PTM reduces rejection risk, while immune activation during rejection protects against malignancy.</p><p><strong>Methods: </strong>We analyzed data from the United Network for Organ Sharing's Organ Procurement and Transplantation Network database (1987-2023) on adult, first-time, single-organ transplant recipients with no prior history of malignancy (in donors or recipients). Landmark analyses at 1, 2, 3, 5, 10, 15, and 20 years post-transplant, Kaplan-Meier analyses, and time-dependent Cox proportional hazards regression models, each incorporating the temporal dimension of outcomes, assessed the association between rejection-induced graft failure (RGF) and PTM. Multivariate models were adjusted for clinical and immunological factors, including immunosuppression regimens.</p><p><strong>Results: </strong>The cohort included 579905 recipients (kidney: 386878; liver: 108390; heart: 45046; lung: 37643; pancreas: 1948) with a mean follow-up of 7.3 years and a median age of 50.6 ± 13.2 years. RGF was associated with a reduction in PTM risk across all time points [hazard ratio (HR) = 0.07-0.20, <i>P</i> < 0.001], even after excluding mortality cases. Kidney transplant recipients exhibited the most pronounced reduction (HR = 0.22, <i>P</i> < 0.001). Conversely, among recipients with PTM, RGF risk decreased across all time points up to 15 years after excluding mortality cases (HR = 0.49-0.80, <i>P</i> < 0.001). This risk reduction was observed in kidney, liver, heart, and lung transplants (HRs = 0.90, 0.21, 0.21, and 0.18, respectively; <i>P</i> < 0.001) but not in pancreas transplants.</p><p><strong>Conclusion: </strong>RGF reduces PTM risk, particularly in kidney transplants, while PTM decreases RGF risk in kidney, liver, heart, and lung transplants.</p>","PeriodicalId":65557,"journal":{"name":"世界移植杂志","volume":"15 2","pages":"102384"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11886299/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5500/wjt.v15.i2.102384","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Advancements in immunosuppressive therapies have improved graft survival by enhancing graft tolerance and preventing organ rejection. However, the risk of malignancy associated with prolonged immunosuppression remains a concern, as it can adversely affect recipients' quality of life and survival. While the link between immunosuppression and increased cancer risk is well-documented, the specific interactions between graft rejection and post-transplant malignancy (PTM) remain poorly understood. Addressing this knowledge gap is crucial for devising immunosuppressive strategies that balance rejection prevention with cancer risk reduction.
Aim: To investigate whether immunosuppression in PTM reduces rejection risk, while immune activation during rejection protects against malignancy.
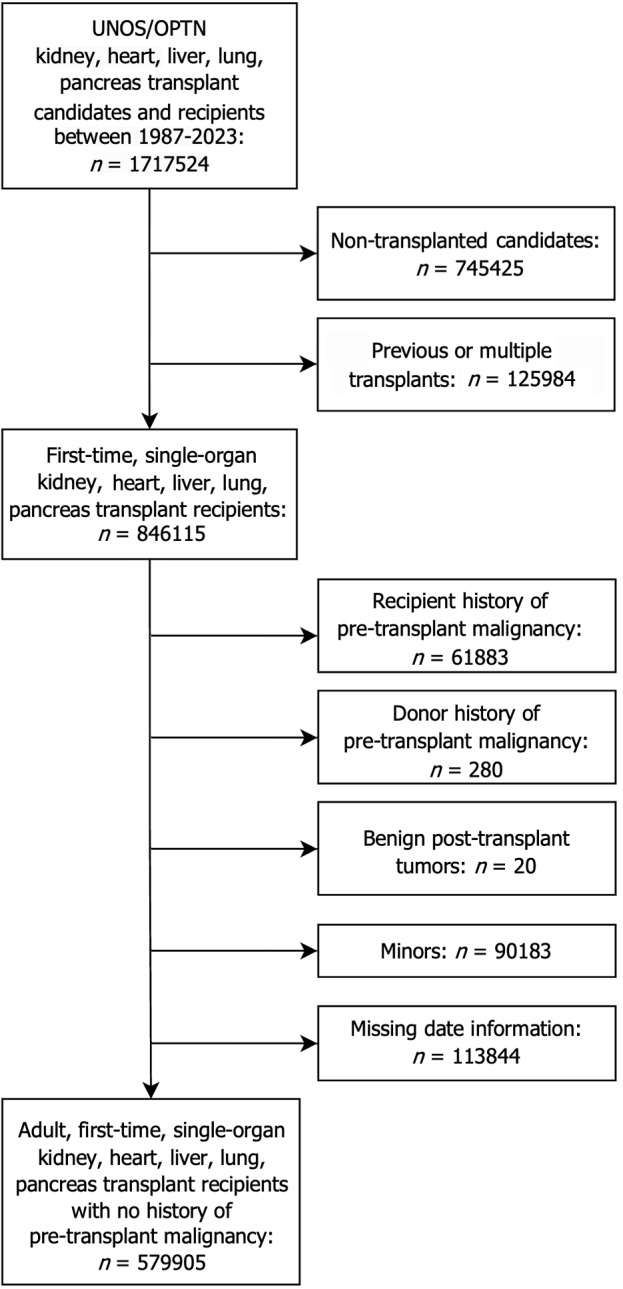
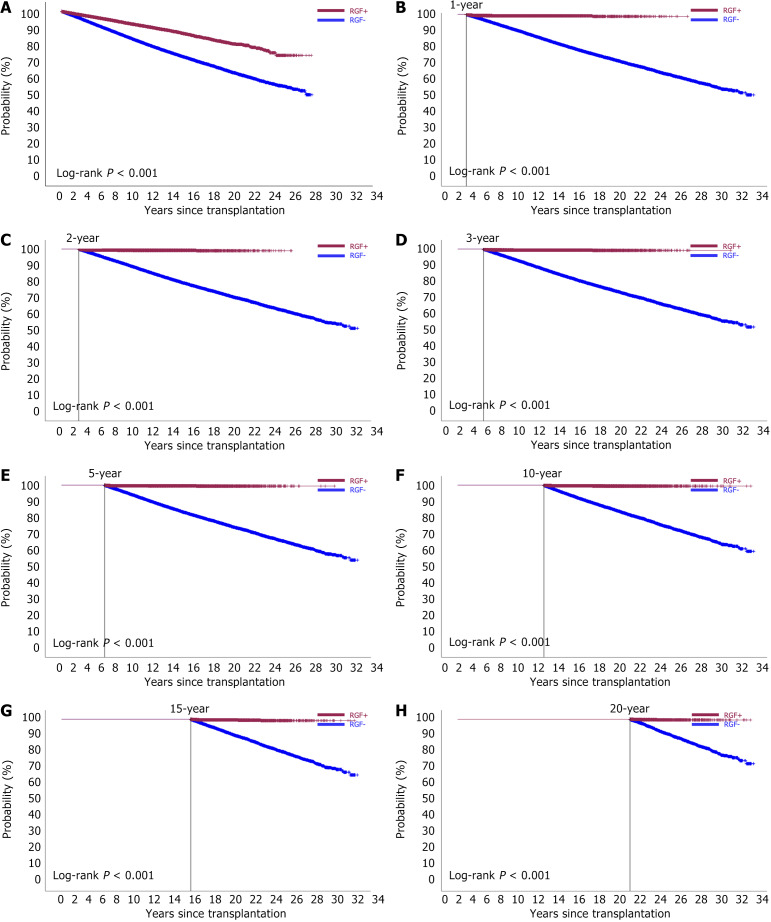
Methods: We analyzed data from the United Network for Organ Sharing's Organ Procurement and Transplantation Network database (1987-2023) on adult, first-time, single-organ transplant recipients with no prior history of malignancy (in donors or recipients). Landmark analyses at 1, 2, 3, 5, 10, 15, and 20 years post-transplant, Kaplan-Meier analyses, and time-dependent Cox proportional hazards regression models, each incorporating the temporal dimension of outcomes, assessed the association between rejection-induced graft failure (RGF) and PTM. Multivariate models were adjusted for clinical and immunological factors, including immunosuppression regimens.
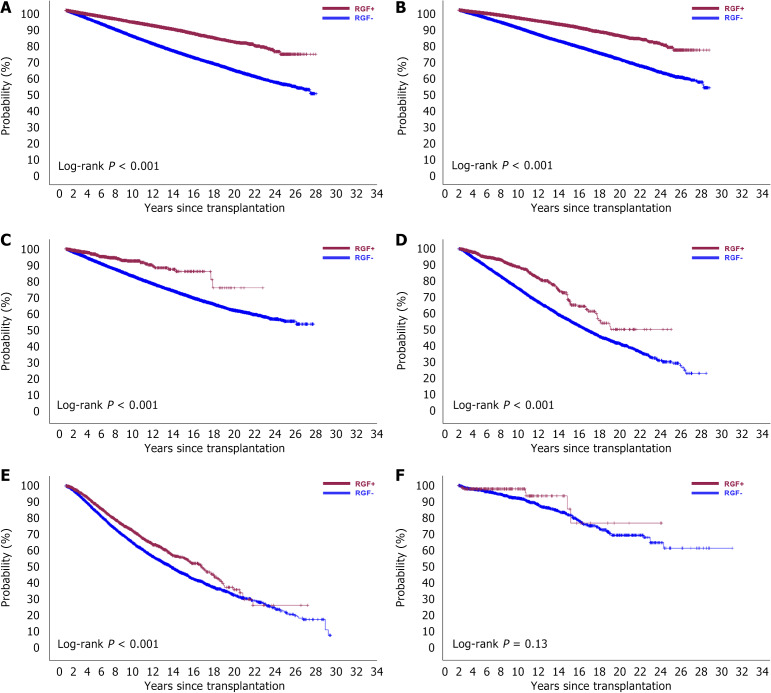
Results: The cohort included 579905 recipients (kidney: 386878; liver: 108390; heart: 45046; lung: 37643; pancreas: 1948) with a mean follow-up of 7.3 years and a median age of 50.6 ± 13.2 years. RGF was associated with a reduction in PTM risk across all time points [hazard ratio (HR) = 0.07-0.20, P < 0.001], even after excluding mortality cases. Kidney transplant recipients exhibited the most pronounced reduction (HR = 0.22, P < 0.001). Conversely, among recipients with PTM, RGF risk decreased across all time points up to 15 years after excluding mortality cases (HR = 0.49-0.80, P < 0.001). This risk reduction was observed in kidney, liver, heart, and lung transplants (HRs = 0.90, 0.21, 0.21, and 0.18, respectively; P < 0.001) but not in pancreas transplants.
Conclusion: RGF reduces PTM risk, particularly in kidney transplants, while PTM decreases RGF risk in kidney, liver, heart, and lung transplants.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


