{"title":"Takayasu's Arteritis with Systemic Lupus Erythematosus: A Case Report.","authors":"Himanshu Jindal, Vinay Suresh, Balakrishnan Kamaraj, Mayank Jha, Nikhil Verma, Awadhesh Kumar Sharma, P Purushothaman, Shubham Kumar, Rachana Mehta, Ranjana Sah, Amogh Verma","doi":"10.1177/11795468251350222","DOIUrl":null,"url":null,"abstract":"<p><p>Takayasu arteritis (TA) is a rare granulomatous vasculitis affecting the aorta and its major branches, while systemic lupus erythematosus (SLE) is a multisystem autoimmune disorder known for vascular and serological involvement. Although both diseases share certain immunopathological pathways, their co-occurrence is exceedingly rare. We report a case of a 44-year-old Indian female with a prior diagnosis of SLE who presented with breathlessness, palpitations, and nodular episcleritis. Cardiovascular evaluation revealed carotid bruit, diminished peripheral pulses, blood pressure discrepancies, and murmurs suggestive of valvular dysfunction. Laboratory investigations demonstrated elevated erythrocyte sedimentation rate, hypochromic microcytic anemia, hypocomplementemia, positive antinuclear and anti-dsDNA antibodies, and proteinuria. Imaging confirmed circumferential thickening of the ascending and descending aorta and occlusive disease in the left carotid system. Based on the 2022 ACR/EULAR classification criteria, a diagnosis of concomitant TA was established. Management included corticosteroids and mycophenolate mofetil, chosen over cyclophosphamide due to borderline renal function and fertility considerations. Despite planning for aortic root replacement, the patient deteriorated and succumbed to complications of severe aortic regurgitation. This case highlights the diagnostic complexities of overlapping autoimmune vasculitides and emphasizes the need for early recognition, rigorous application of classification criteria, and individualized immunosuppressive strategies to optimize outcomes in such rare presentations.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"19 ","pages":"11795468251350222"},"PeriodicalIF":3.3000,"publicationDate":"2025-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12174721/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795468251350222","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
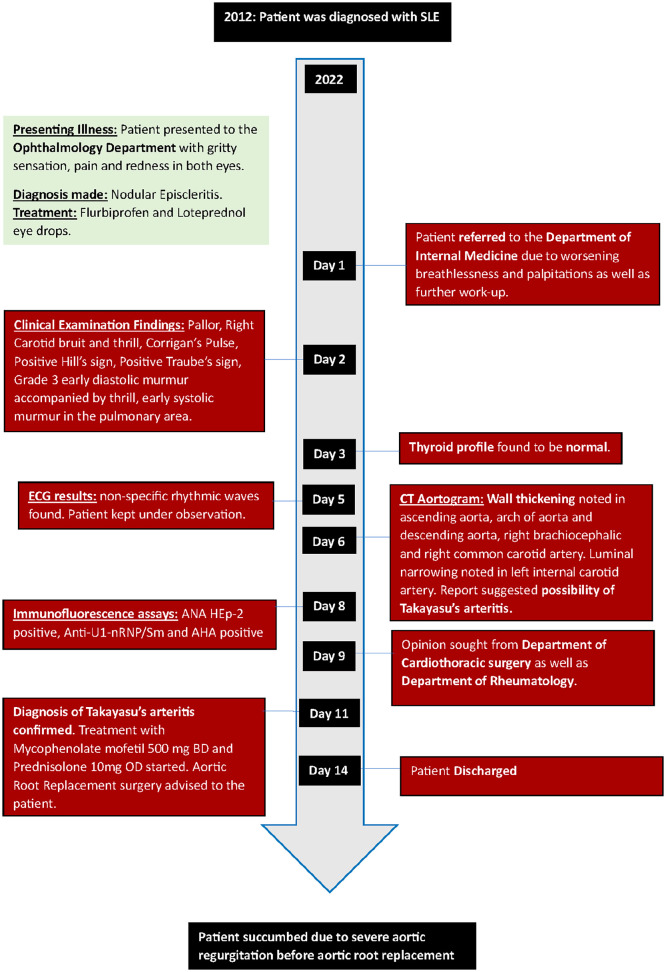
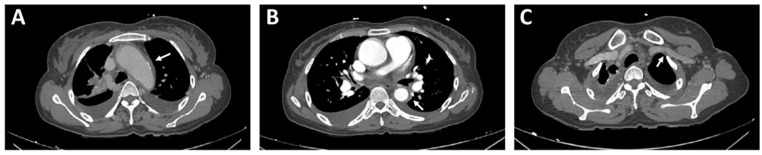
Takayasu arteritis (TA) is a rare granulomatous vasculitis affecting the aorta and its major branches, while systemic lupus erythematosus (SLE) is a multisystem autoimmune disorder known for vascular and serological involvement. Although both diseases share certain immunopathological pathways, their co-occurrence is exceedingly rare. We report a case of a 44-year-old Indian female with a prior diagnosis of SLE who presented with breathlessness, palpitations, and nodular episcleritis. Cardiovascular evaluation revealed carotid bruit, diminished peripheral pulses, blood pressure discrepancies, and murmurs suggestive of valvular dysfunction. Laboratory investigations demonstrated elevated erythrocyte sedimentation rate, hypochromic microcytic anemia, hypocomplementemia, positive antinuclear and anti-dsDNA antibodies, and proteinuria. Imaging confirmed circumferential thickening of the ascending and descending aorta and occlusive disease in the left carotid system. Based on the 2022 ACR/EULAR classification criteria, a diagnosis of concomitant TA was established. Management included corticosteroids and mycophenolate mofetil, chosen over cyclophosphamide due to borderline renal function and fertility considerations. Despite planning for aortic root replacement, the patient deteriorated and succumbed to complications of severe aortic regurgitation. This case highlights the diagnostic complexities of overlapping autoimmune vasculitides and emphasizes the need for early recognition, rigorous application of classification criteria, and individualized immunosuppressive strategies to optimize outcomes in such rare presentations.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


