Optimal timing of laparoscopic cholecystectomy after percutaneous gallbladder drainage in patients with acute calculous cholecystitis: A retrospective comparative study.
Kim-Long Le, Tien-Quang Pham, Phu-Cuong Pham, Minh-Quang Tran, Tri-Nhan Pham, My-Tran Trinh, Nguyen-Khoi Le, Hai Van Nguyen
{"title":"Optimal timing of laparoscopic cholecystectomy after percutaneous gallbladder drainage in patients with acute calculous cholecystitis: A retrospective comparative study.","authors":"Kim-Long Le, Tien-Quang Pham, Phu-Cuong Pham, Minh-Quang Tran, Tri-Nhan Pham, My-Tran Trinh, Nguyen-Khoi Le, Hai Van Nguyen","doi":"10.14701/ahbps.25-062","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Laparoscopic cholecystectomy (LC) is the standard therapy for acute calculous cholecystitis (ACC). However, high-risk patients often require percutaneous gallbladder drainage (PGBD) as a bridge to surgery. The optimal interval between PGBD and LC remains uncertain.</p><p><strong>Methods: </strong>We retrospectively reviewed 177 patients who underwent LC after PGBD for ACC at Nhan dan Gia Dinh Hospital (2018-2024). Patients were stratified by drainage-to-surgery interval: Q1, ≤ 9 days; Q2, 10-17 days; Q3, 18-32 days; Q4, ≥ 32 days. Primary outcomes were operative time, conversion, intraoperative bleeding, postoperative stay, and Clavien-Dindo complications. Multivariable logistic regression was performed after adjusting for age, Charlson Comorbidity Index (CCI), TG18 severity, sex, prior endoscopic retrograde cholangiopancreatography, and Concurrent PGBD and LC during the same admission.</p><p><strong>Results: </strong>Median operative time, conversion rate, and postoperative stay were similar across intervals. Crude bleeding differed significantly (<i>p</i> = 0.019), being the highest in Q4 (68.2%) and the lowest in Q2 (36.4%). Q3 showed the shortest operative time (median: 90 min) and the lowest complication rate (11.4%). In adjusted analysis, only CCI independently predicted bleeding (adjusted odds ratio: 1.42; 95% confidence interval: 1.02-2.03), while timing lost its statistical significance.</p><p><strong>Conclusions: </strong>Scheduling LC 18-32 days after PGBD offers the most balanced surgical profile, whereas delaying beyond 32 days increases bleeding without added benefit. Comorbidity burden rather than calendar interval per se appears to increase bleeding risk. Prospective studies are warranted to confirm the intermediate 2- to 4-week window.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"286-292"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377989/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.25-062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/18 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: Laparoscopic cholecystectomy (LC) is the standard therapy for acute calculous cholecystitis (ACC). However, high-risk patients often require percutaneous gallbladder drainage (PGBD) as a bridge to surgery. The optimal interval between PGBD and LC remains uncertain.
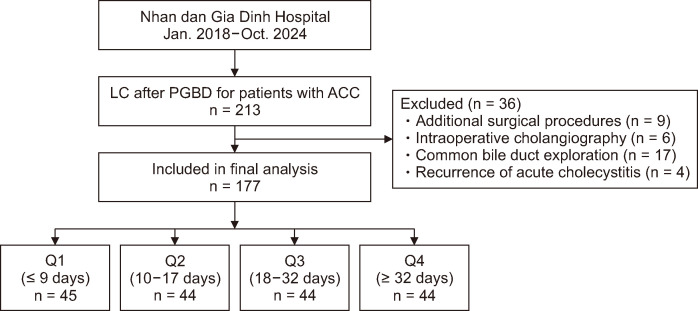
Methods: We retrospectively reviewed 177 patients who underwent LC after PGBD for ACC at Nhan dan Gia Dinh Hospital (2018-2024). Patients were stratified by drainage-to-surgery interval: Q1, ≤ 9 days; Q2, 10-17 days; Q3, 18-32 days; Q4, ≥ 32 days. Primary outcomes were operative time, conversion, intraoperative bleeding, postoperative stay, and Clavien-Dindo complications. Multivariable logistic regression was performed after adjusting for age, Charlson Comorbidity Index (CCI), TG18 severity, sex, prior endoscopic retrograde cholangiopancreatography, and Concurrent PGBD and LC during the same admission.
Results: Median operative time, conversion rate, and postoperative stay were similar across intervals. Crude bleeding differed significantly (p = 0.019), being the highest in Q4 (68.2%) and the lowest in Q2 (36.4%). Q3 showed the shortest operative time (median: 90 min) and the lowest complication rate (11.4%). In adjusted analysis, only CCI independently predicted bleeding (adjusted odds ratio: 1.42; 95% confidence interval: 1.02-2.03), while timing lost its statistical significance.
Conclusions: Scheduling LC 18-32 days after PGBD offers the most balanced surgical profile, whereas delaying beyond 32 days increases bleeding without added benefit. Comorbidity burden rather than calendar interval per se appears to increase bleeding risk. Prospective studies are warranted to confirm the intermediate 2- to 4-week window.
背景/目的:腹腔镜胆囊切除术(LC)是急性结石性胆囊炎(ACC)的标准治疗。然而,高风险患者往往需要经皮胆囊引流(PGBD)作为手术的桥梁。PGBD和LC之间的最优间隔仍然不确定。方法:我们回顾性分析了Nhan dan Gia Dinh医院(2018-2024)177例因ACC而接受PGBD后LC治疗的患者。患者按引流至手术间隔进行分层:Q1,≤9天;Q2: 10-17天;Q3, 18-32天;Q4,≥32天。主要结局为手术时间、转换、术中出血、术后住院时间和Clavien-Dindo并发症。在调整年龄、Charlson合并症指数(CCI)、TG18严重程度、性别、既往内镜逆行胆管造影以及同一入院期间并发PGBD和LC后,进行多变量logistic回归。结果:中位手术时间、转换率和术后住院时间在不同时间间隔相似。原油放量差异显著(p = 0.019),第四季度最高(68.2%),第二季度最低(36.4%)。Q3手术时间最短(中位90 min),并发症发生率最低(11.4%)。在校正分析中,只有CCI独立预测出血(校正优势比:1.42;95%置信区间:1.02-2.03),而时间则失去了统计学意义。结论:在PGBD后18-32天安排LC提供了最平衡的手术方案,而延迟超过32天会增加出血,但没有额外的好处。合并症负担而不是日历间隔本身似乎增加了出血风险。有必要进行前瞻性研究,以确认中间2至4周的窗口期。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


