Lindsey Jackson, Jacob Poynter, Maryam Rahman, Tara Massini, Si Chen
{"title":"Management of Rare Temporomandibular Joint Cysts with Intracranial Extension: A Case Series and Literature Review.","authors":"Lindsey Jackson, Jacob Poynter, Maryam Rahman, Tara Massini, Si Chen","doi":"10.1055/a-2620-3584","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Temporomandibular joint (TMJ) cysts extending through the skull base into the middle cranial fossa (MCF) are rare, with limited data on clinical progression and treatment. This study retrospectively analyzed three cases of TMJ cysts with MCF extension managed by a multidisciplinary team. Clinical presentation, imaging, surgical resection, outcomes, and a literature review are presented.</p><p><strong>Case presentations: </strong>Three patients presenting with otalgia and TMJ tenderness were found to have intracranial cysts communicating with the TMJ. Two patients had been transferred with suspected intracranial abscesses; one presented for workup of headache and trigeminal neuralgia. All three demonstrated elevation of inflammatory markers. Two patients had TMJ aspiration, notable for leukocytosis and crystalline deposition, another had frank purulence. One patient demonstrated pneumocephalus within the cyst on imaging. The intracranial cysts ranged from 1.2 to 3.3 cm in maximum diameter, with their bony defects ranging from <1 to 4 mm. Two patients underwent craniotomy, cyst resection, and repair of the middle fossa defect, while the third opted for observation. Pathology of the white gelatinous fluid within the two resected growths demonstrated benign cysts.</p><p><strong>Conclusion: </strong>TMJ cysts with intracranial extension, while rare, require careful differentiation from intracranial abscesses. Surgical urgency may be indicated in cases demonstrating clinical signs of infection. Additionally, TMJ cysts with intracranial extension benefit from surgical removal and skull base repair to relieve symptoms and prevent future complications.</p>","PeriodicalId":44256,"journal":{"name":"Journal of Neurological Surgery Reports","volume":"86 2","pages":"e127-e132"},"PeriodicalIF":0.7000,"publicationDate":"2025-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12173542/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurological Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2620-3584","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Temporomandibular joint (TMJ) cysts extending through the skull base into the middle cranial fossa (MCF) are rare, with limited data on clinical progression and treatment. This study retrospectively analyzed three cases of TMJ cysts with MCF extension managed by a multidisciplinary team. Clinical presentation, imaging, surgical resection, outcomes, and a literature review are presented.
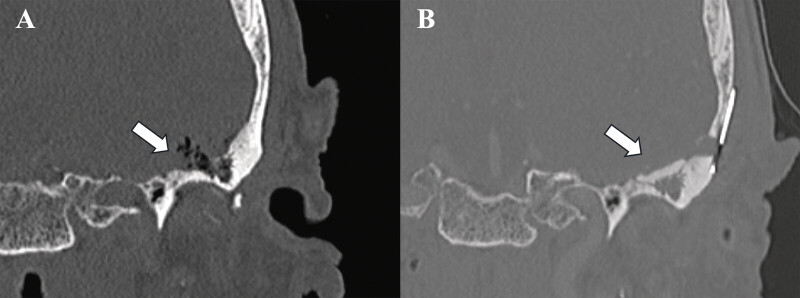
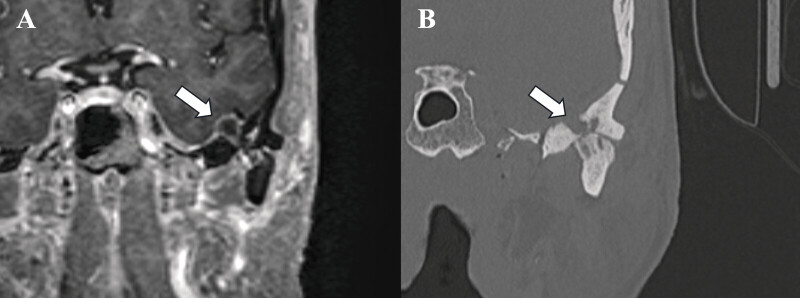
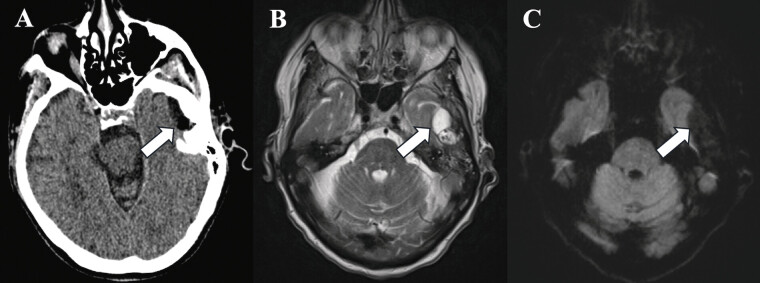
Case presentations: Three patients presenting with otalgia and TMJ tenderness were found to have intracranial cysts communicating with the TMJ. Two patients had been transferred with suspected intracranial abscesses; one presented for workup of headache and trigeminal neuralgia. All three demonstrated elevation of inflammatory markers. Two patients had TMJ aspiration, notable for leukocytosis and crystalline deposition, another had frank purulence. One patient demonstrated pneumocephalus within the cyst on imaging. The intracranial cysts ranged from 1.2 to 3.3 cm in maximum diameter, with their bony defects ranging from <1 to 4 mm. Two patients underwent craniotomy, cyst resection, and repair of the middle fossa defect, while the third opted for observation. Pathology of the white gelatinous fluid within the two resected growths demonstrated benign cysts.
Conclusion: TMJ cysts with intracranial extension, while rare, require careful differentiation from intracranial abscesses. Surgical urgency may be indicated in cases demonstrating clinical signs of infection. Additionally, TMJ cysts with intracranial extension benefit from surgical removal and skull base repair to relieve symptoms and prevent future complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


