Dre E Steinwehr, Jena M Gales, Anya R de Leeuw, Derek S Anderson, Christopher R Cunningham, Aaron A H Smith
{"title":"Biopsy Confirmed Skin Drug Eruption in Setting of Ticagrelor Use.","authors":"Dre E Steinwehr, Jena M Gales, Anya R de Leeuw, Derek S Anderson, Christopher R Cunningham, Aaron A H Smith","doi":"10.1177/23247096251350547","DOIUrl":null,"url":null,"abstract":"<p><p>When there is concern that a rash may be a drug eruption reaction, there are many well-known culprits such as antibiotics and phenytoin. When an uncommon or previously unknown offending medication is being considered to have caused a drug eruption, diagnostic skin biopsy can help confirm the diagnosis. Our patient is a 54-year-old female with past medical history of prediabetes and obesity. She had ST segment-elevation myocardial infarction that was treated appropriately with timely percutaneous coronary intervention, which included angioplasty and drug-eluting stent placement. She was maintained on treatment regimen, and over the next 3 months, she developed a worsening maculopapular rash across her torso and upper extremities. Her biopsy showed superficial and mid-dermal perivascular lymphohistiocytic inflammation with focal spongiosis and scattered eosinophils, a common pathologic finding seen in drug eruptions. Although the patient was not taking any well-known offending agents, her ticagrelor was discontinued and she was transitioned to clopidogrel. Shortly after the transition, the patient's drug rash resolved without recurrence. Drug eruptions are a common etiology for rashes leading to presentation in primary care clinics. Our patient illustrates an exceedingly rare case of ticagrelor-induced drug reaction, as a review of the literature shows only 2 previously published case reports.</p>","PeriodicalId":16198,"journal":{"name":"Journal of investigative medicine high impact case reports","volume":"13 ","pages":"23247096251350547"},"PeriodicalIF":0.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12177242/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of investigative medicine high impact case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23247096251350547","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
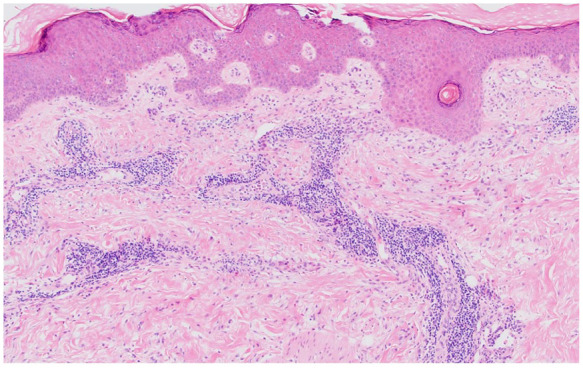
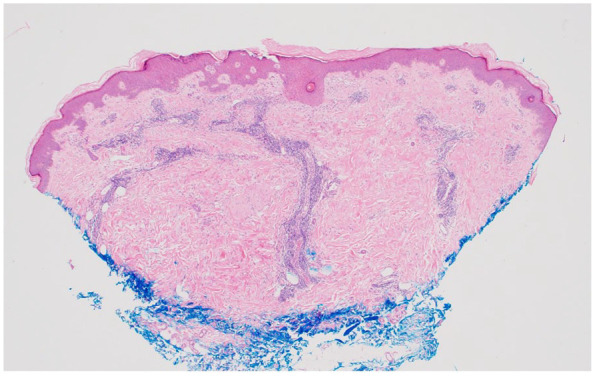
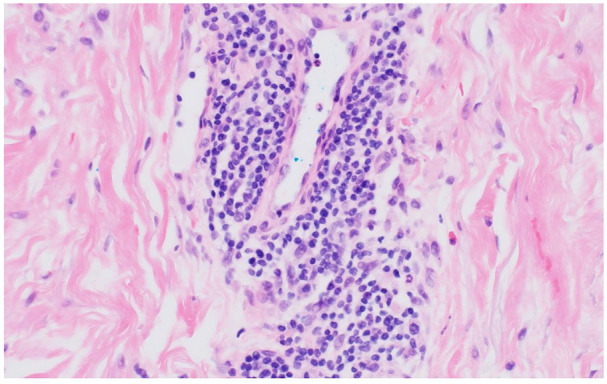
When there is concern that a rash may be a drug eruption reaction, there are many well-known culprits such as antibiotics and phenytoin. When an uncommon or previously unknown offending medication is being considered to have caused a drug eruption, diagnostic skin biopsy can help confirm the diagnosis. Our patient is a 54-year-old female with past medical history of prediabetes and obesity. She had ST segment-elevation myocardial infarction that was treated appropriately with timely percutaneous coronary intervention, which included angioplasty and drug-eluting stent placement. She was maintained on treatment regimen, and over the next 3 months, she developed a worsening maculopapular rash across her torso and upper extremities. Her biopsy showed superficial and mid-dermal perivascular lymphohistiocytic inflammation with focal spongiosis and scattered eosinophils, a common pathologic finding seen in drug eruptions. Although the patient was not taking any well-known offending agents, her ticagrelor was discontinued and she was transitioned to clopidogrel. Shortly after the transition, the patient's drug rash resolved without recurrence. Drug eruptions are a common etiology for rashes leading to presentation in primary care clinics. Our patient illustrates an exceedingly rare case of ticagrelor-induced drug reaction, as a review of the literature shows only 2 previously published case reports.
期刊介绍:
The AFMR is committed to enhancing the training and career development of our members and to furthering its mission to facilitate the conduct of research to improve medical care. Case reports represent an important avenue for trainees (interns, residents, and fellows) and early-stage faculty to demonstrate productive, scholarly activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


