Implementing electronic health record-based anxiety and depression screening in an epilepsy clinic: Theory-based implementation strategy and pre-post quantitative outcomes using Reach, Effectiveness, Adoption, Implementation, and Maintenance.
Heidi M Munger Clary, Halley B Alexander, Sabina Gesell, Mingyu Wan, Kelly R Conner, Cormac O'Donovan, Jane Boggs, Christian Robles, Maria Sam, Jerryl Christopher, Christina Marini, Beverly M Snively
{"title":"Implementing electronic health record-based anxiety and depression screening in an epilepsy clinic: Theory-based implementation strategy and pre-post quantitative outcomes using Reach, Effectiveness, Adoption, Implementation, and Maintenance.","authors":"Heidi M Munger Clary, Halley B Alexander, Sabina Gesell, Mingyu Wan, Kelly R Conner, Cormac O'Donovan, Jane Boggs, Christian Robles, Maria Sam, Jerryl Christopher, Christina Marini, Beverly M Snively","doi":"10.1017/cts.2025.74","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Anxiety and depression in epilepsy are common and impactful. Screening with validated measures at every epilepsy visit is a quality measure, yet screening remains limited due to time constraints.</p><p><strong>Methods: </strong>This study aimed to develop an implementation strategy for anxiety and depression screening at an epilepsy center and evaluate it in a pre-post design with RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance). Guided by the Capability, Opportunity, Motivation-Behavior behavior change wheel framework, the strategy incorporated electronic health record tools and support staff activation of electronic screeners during visit check-in. Outcomes were evaluated over five months post-implementation and compared with two 3-month pre-implementation timeframes.</p><p><strong>Results: </strong>Post-implementation, 29.2% of 943 visits met the anxiety and depression screening quality measure, a significant increase from 12.6% immediately pre-implementation (p < 0.0001) and 6.28% before any screening interventions (p < 0.0001). Patients who completed electronic screeners post-implementation were younger than non-completers (mean 39.3 vs. 43.4 years, <i>p</i> = 0.001) and more likely to be white than other race/ethnicity categories (p = 0.002). There was substantial variability in screening rates among clinic staff (0-80% for support staff, 10.1-55.3% for providers), with higher screening among neurology support staff than temporary staff. Only 0.23% of post-implementation visits had screeners initiated but left incomplete. A shift to virtual visits during COVID-19 complicated Maintenance.</p><p><strong>Conclusions: </strong>This framework-based implementation strategy effectively increased screening rates by epilepsy specialists, though challenges remain, including variability across clinic team members and lower reach among older and non-white patients. This study describes a feasible strategy for epilepsy centers to use for improved performance on an American Academy of Neurology quality measure (depression and anxiety screening for patients with epilepsy).</p>","PeriodicalId":15529,"journal":{"name":"Journal of Clinical and Translational Science","volume":"9 1","pages":"e108"},"PeriodicalIF":2.0000,"publicationDate":"2025-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12171918/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/cts.2025.74","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Anxiety and depression in epilepsy are common and impactful. Screening with validated measures at every epilepsy visit is a quality measure, yet screening remains limited due to time constraints.
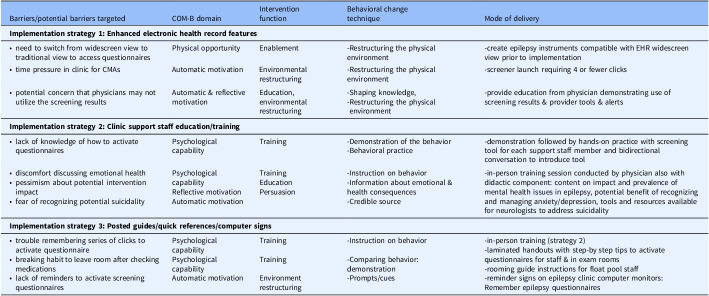
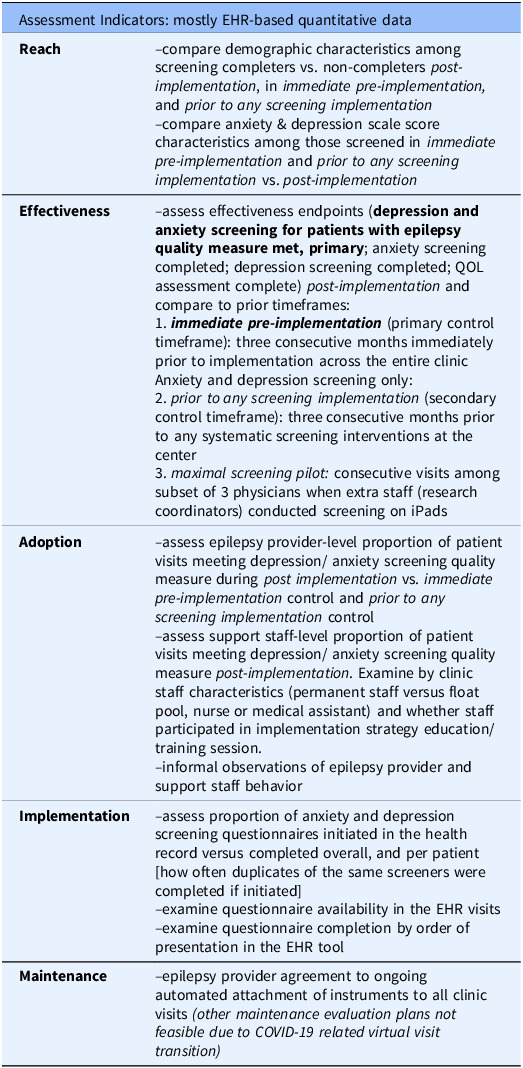
Methods: This study aimed to develop an implementation strategy for anxiety and depression screening at an epilepsy center and evaluate it in a pre-post design with RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance). Guided by the Capability, Opportunity, Motivation-Behavior behavior change wheel framework, the strategy incorporated electronic health record tools and support staff activation of electronic screeners during visit check-in. Outcomes were evaluated over five months post-implementation and compared with two 3-month pre-implementation timeframes.
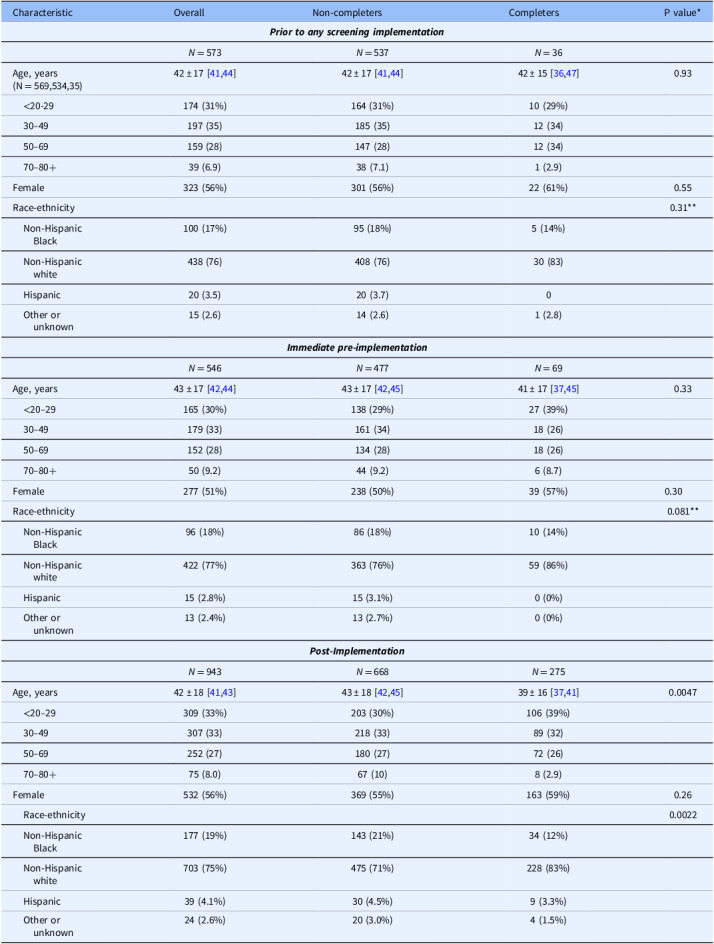
Results: Post-implementation, 29.2% of 943 visits met the anxiety and depression screening quality measure, a significant increase from 12.6% immediately pre-implementation (p < 0.0001) and 6.28% before any screening interventions (p < 0.0001). Patients who completed electronic screeners post-implementation were younger than non-completers (mean 39.3 vs. 43.4 years, p = 0.001) and more likely to be white than other race/ethnicity categories (p = 0.002). There was substantial variability in screening rates among clinic staff (0-80% for support staff, 10.1-55.3% for providers), with higher screening among neurology support staff than temporary staff. Only 0.23% of post-implementation visits had screeners initiated but left incomplete. A shift to virtual visits during COVID-19 complicated Maintenance.
Conclusions: This framework-based implementation strategy effectively increased screening rates by epilepsy specialists, though challenges remain, including variability across clinic team members and lower reach among older and non-white patients. This study describes a feasible strategy for epilepsy centers to use for improved performance on an American Academy of Neurology quality measure (depression and anxiety screening for patients with epilepsy).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


