Omar E S Mostafa, Shafquat Zaman, Maymunah Malik, Prajeesh Kumar, Lalit Kumar, Akinfemi Akingboye, Diwakar Sarma, Rajeev Peravali
{"title":"Clinical outcomes of conventional versus extended mesenteric resection in limited ileo-colonic Crohn's disease: a systematic review and meta-analysis.","authors":"Omar E S Mostafa, Shafquat Zaman, Maymunah Malik, Prajeesh Kumar, Lalit Kumar, Akinfemi Akingboye, Diwakar Sarma, Rajeev Peravali","doi":"10.1007/s00384-025-04937-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of intestinal mesentery and the extent of its resection as a determinant of outcomes post-bowel resection in Crohn's disease (CD) remains a subject of debate. We evaluated outcomes of conventional mesenteric resection (CMR) and compared it with extended mesenteric resection (EMR) in patients undergoing ileo-colic excision for limited ileo-colonic CD.</p><p><strong>Methods: </strong>A comprehensive search was conducted in accordance with PRISMA guidelines using Medline, Embase, PubMed, and Cochrane databases. Comparative studies of patients with limited ileo-colonic CD undergoing CMR and EMR for ileo-colic resection were included. Studies comparing anastomotic techniques, single-arm, case reports/series, study protocols and editorials were excluded. Primary outcomes were disease recurrence and re-operation. Secondary outcomes included post-operative complications, intra-operative blood loss, length of stay, total operative time and re-admission rate. Meta-analysis was performed using Cochrane RevMan Web on outcomes reported by two or more studies. Combined overall effect sizes were calculated using random-effects model and the Newcastle-Ottawa Scale and Cochrane risk-of-bias tools were used to assess bias.</p><p><strong>Results: </strong>Five studies met our inclusion criteria (four retrospective cohort studies; one randomised controlled trial (RCT)) with a total of 4,358 patients (EMR: 993 vs. CMR: 3,365). No statistical difference was observed across any of the analysed outcomes: disease recurrence [OR: 0.49 CI 0.21-1.16, P = 0.10], re-operation [OR: 0.33 CI 0.06-1.65, P = 0.17], intra-operative blood loss [MD: -18.71 CI -76.65-39.23, P = 0.53], anastomotic leak [OR: 0.98 CI 0.34-2.82, P = 0.97], length of stay [MD: -0.06 CI -0.59-0.48, P = 0.83], post-operative morbidity [OR: 1.01 CI 0.82-1.24, P = 0.95], blood transfusion [OR: 1.16 CI 0.84-1.59, P = 0.36], Clavien-Dindo III + complications [OR: 0.83 CI 0.5-1.38, P = 0.47], post-operative ileus [OR: 0.97 CI 0.27-3.50, P = 0.96], intra-abdominal bleeding [OR: 0.85 CI 0.22-3.26, P = 0.81], re-admission [OR: 0.65 CI 0.24-1.78, P = 0.40], surgical site infection [OR: 1.00 CI 0.77-1.30, P = 0.99], post-operative adjuvant or prophylactic therapy [OR: 0.90 CI 0.54-1.51, P = 0.69] and total operative time [MD: 0.38 CI -4.42-5.19, P = 0.88].</p><p><strong>Conclusion: </strong>Performing EMR during ileo-colic resection for patients with limited ileo-colonic CD does not seem to confer any additional benefit to conventional (limited resection) approaches. Robust, well-designed, large-scale RCTs are needed to better compare these techniques and demonstrate superiority in clinical outcomes.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"144"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12174243/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04937-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of intestinal mesentery and the extent of its resection as a determinant of outcomes post-bowel resection in Crohn's disease (CD) remains a subject of debate. We evaluated outcomes of conventional mesenteric resection (CMR) and compared it with extended mesenteric resection (EMR) in patients undergoing ileo-colic excision for limited ileo-colonic CD.
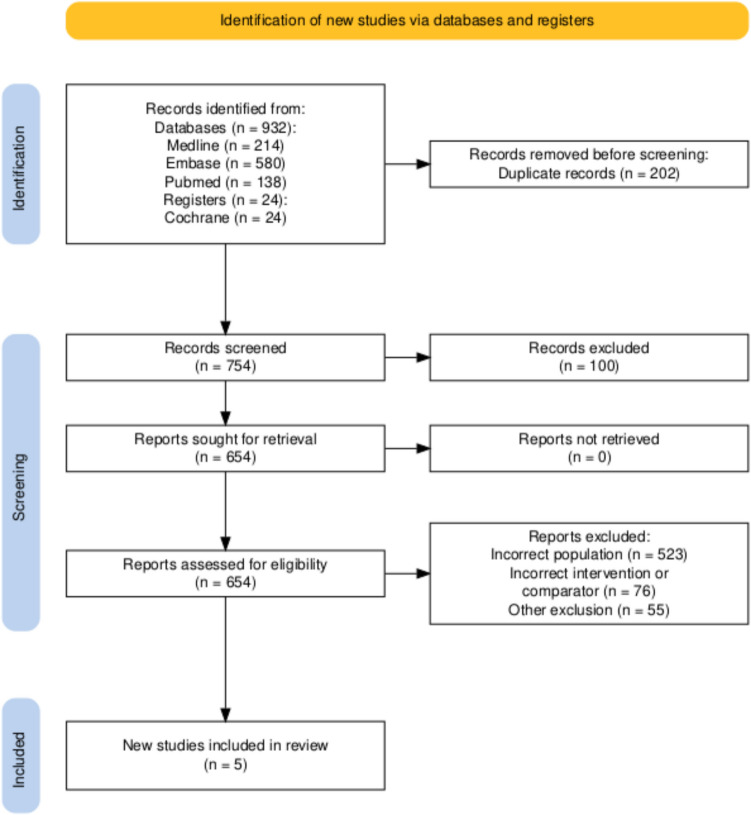
Methods: A comprehensive search was conducted in accordance with PRISMA guidelines using Medline, Embase, PubMed, and Cochrane databases. Comparative studies of patients with limited ileo-colonic CD undergoing CMR and EMR for ileo-colic resection were included. Studies comparing anastomotic techniques, single-arm, case reports/series, study protocols and editorials were excluded. Primary outcomes were disease recurrence and re-operation. Secondary outcomes included post-operative complications, intra-operative blood loss, length of stay, total operative time and re-admission rate. Meta-analysis was performed using Cochrane RevMan Web on outcomes reported by two or more studies. Combined overall effect sizes were calculated using random-effects model and the Newcastle-Ottawa Scale and Cochrane risk-of-bias tools were used to assess bias.
Results: Five studies met our inclusion criteria (four retrospective cohort studies; one randomised controlled trial (RCT)) with a total of 4,358 patients (EMR: 993 vs. CMR: 3,365). No statistical difference was observed across any of the analysed outcomes: disease recurrence [OR: 0.49 CI 0.21-1.16, P = 0.10], re-operation [OR: 0.33 CI 0.06-1.65, P = 0.17], intra-operative blood loss [MD: -18.71 CI -76.65-39.23, P = 0.53], anastomotic leak [OR: 0.98 CI 0.34-2.82, P = 0.97], length of stay [MD: -0.06 CI -0.59-0.48, P = 0.83], post-operative morbidity [OR: 1.01 CI 0.82-1.24, P = 0.95], blood transfusion [OR: 1.16 CI 0.84-1.59, P = 0.36], Clavien-Dindo III + complications [OR: 0.83 CI 0.5-1.38, P = 0.47], post-operative ileus [OR: 0.97 CI 0.27-3.50, P = 0.96], intra-abdominal bleeding [OR: 0.85 CI 0.22-3.26, P = 0.81], re-admission [OR: 0.65 CI 0.24-1.78, P = 0.40], surgical site infection [OR: 1.00 CI 0.77-1.30, P = 0.99], post-operative adjuvant or prophylactic therapy [OR: 0.90 CI 0.54-1.51, P = 0.69] and total operative time [MD: 0.38 CI -4.42-5.19, P = 0.88].
Conclusion: Performing EMR during ileo-colic resection for patients with limited ileo-colonic CD does not seem to confer any additional benefit to conventional (limited resection) approaches. Robust, well-designed, large-scale RCTs are needed to better compare these techniques and demonstrate superiority in clinical outcomes.
背景:肠肠系膜的作用及其切除程度作为肠切除术后克罗恩病(CD)预后的决定因素仍然是一个有争议的主题。我们评估了常规肠系膜切除术(CMR)的结果,并将其与扩展肠系膜切除术(EMR)在接受局限性回肠结肠cd的回肠结肠切除术患者中的效果进行了比较。方法:根据PRISMA指南,使用Medline, Embase, PubMed和Cochrane数据库进行了全面的检索。对局限性回肠-结肠CD患者进行CMR和EMR回肠-结肠切除术的比较研究。比较吻合技术、单臂、病例报告/系列、研究方案和社论的研究被排除。主要结果为疾病复发和再次手术。次要结局包括术后并发症、术中出血量、住院时间、总手术时间和再入院率。使用Cochrane RevMan Web对两项或两项以上研究报告的结果进行meta分析。使用随机效应模型计算综合总体效应大小,并使用纽卡斯尔-渥太华量表和Cochrane偏倚风险工具评估偏倚。结果:5项研究符合我们的纳入标准(4项回顾性队列研究;一项随机对照试验(RCT),共有4358名患者(EMR: 993对CMR: 3365)。各分析结果间无统计学差异:疾病复发[OR: 0.49 CI 0.21-1.16, P = 0.10]、再手术[OR: 0.33 CI 0.06-1.65, P = 0.17]、术中出血量[MD: -18.71 CI -76.65-39.23, P = 0.53]、吻合口漏[OR: 0.98 CI 0.34-2.82, P = 0.97]、住院时间[MD: -0.06 CI -0.59-0.48, P = 0.83]、术后发病率[OR: 1.01 CI 0.82-1.24, P = 0.95]、输血[OR:1.16 CI 0.84-1.59, P = 0.36], Clavien-Dindo III +并发症[OR: 0.83 CI 0.5-1.38, P = 0.47],术后肠梗阻[OR: 0.97 CI 0.27-3.50, P = 0.96],腹腔内出血[OR: 0.85 CI 0.22-3.26, P = 0.81],再入院[OR: 0.65 CI 0.24-1.78, P = 0.40],手术部位感染[OR: 1.00 CI 0.77-1.30, P = 0.99],术后辅助或预防性治疗[OR: 0.90 CI 0.54-1.51, P = 0.69]和总手术时间[MD: 0.38 CI -4.42-5.19, P = 0.88]。结论:对于局限性回肠结肠CD患者,在回肠结肠切除术期间进行EMR似乎没有比传统(有限切除)方法带来任何额外的好处。需要稳健、设计良好、大规模的随机对照试验来更好地比较这些技术,并证明它们在临床结果上的优势。
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


