Left ventricular systolic longitudinal strain in mechanically ventilated patients in the intensive care unit: assessment of global and chamber reproducibility.
Matías Pécora, Piero Pastorini, Roberto Farolini, Gastón Burghi, F Javier Hurtado
{"title":"Left ventricular systolic longitudinal strain in mechanically ventilated patients in the intensive care unit: assessment of global and chamber reproducibility.","authors":"Matías Pécora, Piero Pastorini, Roberto Farolini, Gastón Burghi, F Javier Hurtado","doi":"10.1186/s40635-025-00770-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In the intensive care unit (ICU), left ventricular systolic function is traditionally assessed by measuring the left ventricular ejection fraction (LVEF). Recently, left ventricular global systolic longitudinal strain (SL-S) has emerged as a more sensitive marker of myocardial function in this setting. However, obtaining high-quality echocardiographic images remains a significant challenge, particularly in patients undergoing invasive mechanical ventilation (IMV), and data on the feasibility and reproducibility of these measurements in critically ill patients are limited.</p><p><strong>Objective: </strong>To assess the feasibility and reproducibility (both global and per chamber) of SL-S and LVEF (both manual and automatic) in ICU patients under IMV.</p><p><strong>Materials and methods: </strong>Thirty ICU patients receiving IMV were randomly selected. The feasibility and reproducibility of SL-S (global and per chamber) and LVEF were assessed using both manual and automatic methods. The analysis was performed using the intraclass correlation coefficient (ICC) with its 95% confidence interval (CI), and Bland-Altman analysis (BA), which reported the mean difference and limits of agreement (lower-upper limits of agreement).</p><p><strong>Results: </strong>SL-S was feasible in 70% of patients and demonstrated excellent intra- and interobserver reproducibility for both manual and automatic methods. Intraobserver reproducibility for automatic SL-S: ICC 0.97 (CI: 0.94-0.99), BA 0.26 (-1.89 to 2.40) and interobserver reproducibility: ICC 0.96 (CI: 0.92-0.98), and BA 0.53 (-2.41 to 3.47). The reproducibility of manual SL-S was comparable to automatic measurements. Additionally, the reproducibility per chamber was excellent. LVEF was feasible in 80% of patients. Manual LVEF (Simpson's biplane) reproducibility demonstrated good reproducibility: intraobserver ICC: 0.82 (CI: 0.48-0.93), BA -5.00 (-19.70 to 9.70); interobserver ICC 0.78 (CI: 0.55-0.91), BA 7.50 (-5.40 to 20.40). Automatic LVEF (auto-LVEF) demonstrated excellent reproducibility: intraobserver ICC: 0.94 (CI: 0.86-0.98), BA -0.95 (-10.02 to 8.13); and interobserver ICC: 0.94 (CI: 0.87-0.97), BA 1.75 (-6.38 to 10.33).</p><p><strong>Conclusion: </strong>SL-S (global and per chamber) and auto-LVEF were feasible and showed excellent reproducibility. LVEF demonstrated the highest feasibility, while SL-S exhibited the greatest reproducibility. These parameters may represent a useful tool in the evaluation of LV function in ICU patients under IMV.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"62"},"PeriodicalIF":2.8000,"publicationDate":"2025-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12173981/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00770-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: In the intensive care unit (ICU), left ventricular systolic function is traditionally assessed by measuring the left ventricular ejection fraction (LVEF). Recently, left ventricular global systolic longitudinal strain (SL-S) has emerged as a more sensitive marker of myocardial function in this setting. However, obtaining high-quality echocardiographic images remains a significant challenge, particularly in patients undergoing invasive mechanical ventilation (IMV), and data on the feasibility and reproducibility of these measurements in critically ill patients are limited.
Objective: To assess the feasibility and reproducibility (both global and per chamber) of SL-S and LVEF (both manual and automatic) in ICU patients under IMV.
Materials and methods: Thirty ICU patients receiving IMV were randomly selected. The feasibility and reproducibility of SL-S (global and per chamber) and LVEF were assessed using both manual and automatic methods. The analysis was performed using the intraclass correlation coefficient (ICC) with its 95% confidence interval (CI), and Bland-Altman analysis (BA), which reported the mean difference and limits of agreement (lower-upper limits of agreement).
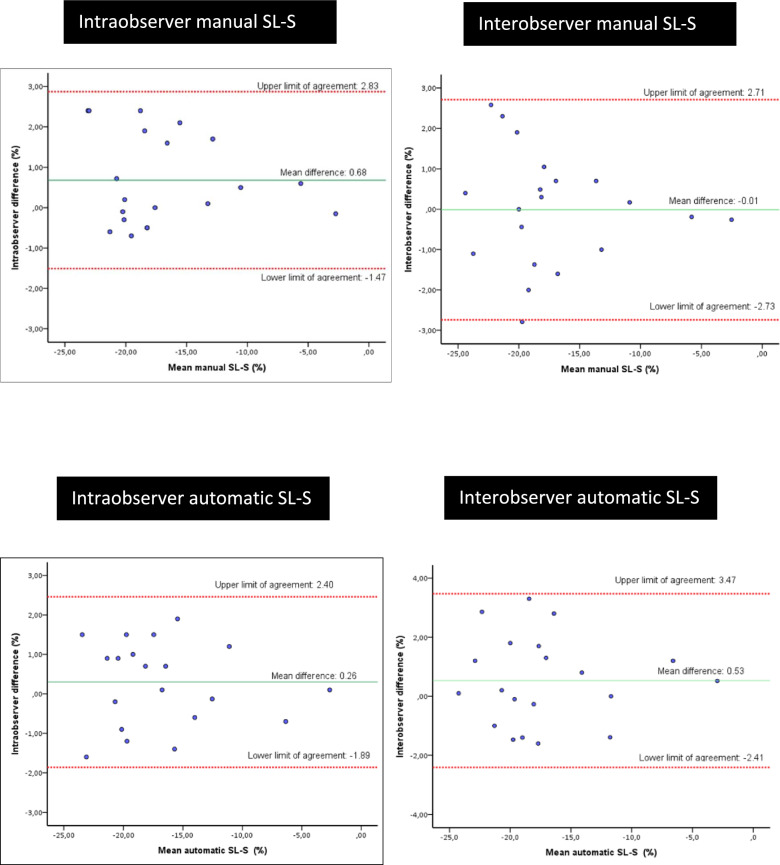
Results: SL-S was feasible in 70% of patients and demonstrated excellent intra- and interobserver reproducibility for both manual and automatic methods. Intraobserver reproducibility for automatic SL-S: ICC 0.97 (CI: 0.94-0.99), BA 0.26 (-1.89 to 2.40) and interobserver reproducibility: ICC 0.96 (CI: 0.92-0.98), and BA 0.53 (-2.41 to 3.47). The reproducibility of manual SL-S was comparable to automatic measurements. Additionally, the reproducibility per chamber was excellent. LVEF was feasible in 80% of patients. Manual LVEF (Simpson's biplane) reproducibility demonstrated good reproducibility: intraobserver ICC: 0.82 (CI: 0.48-0.93), BA -5.00 (-19.70 to 9.70); interobserver ICC 0.78 (CI: 0.55-0.91), BA 7.50 (-5.40 to 20.40). Automatic LVEF (auto-LVEF) demonstrated excellent reproducibility: intraobserver ICC: 0.94 (CI: 0.86-0.98), BA -0.95 (-10.02 to 8.13); and interobserver ICC: 0.94 (CI: 0.87-0.97), BA 1.75 (-6.38 to 10.33).
Conclusion: SL-S (global and per chamber) and auto-LVEF were feasible and showed excellent reproducibility. LVEF demonstrated the highest feasibility, while SL-S exhibited the greatest reproducibility. These parameters may represent a useful tool in the evaluation of LV function in ICU patients under IMV.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


