Simple assessment for rotation of the forearm using three-dimensional bone models
IF 1.4
3区 医学
Q4 ENGINEERING, BIOMEDICAL
引用次数: 0
Abstract
Background
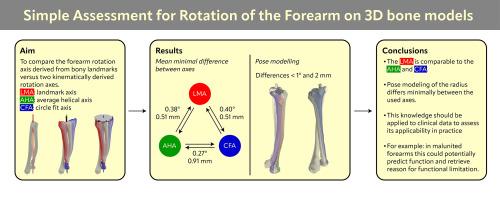
Dynamic medical imaging can determine the cause of rotational impairment in the forearm. However, it has drawbacks depending on the image modality used, related to radiation dose, the need for specialized equipment, and the labor intensity involved in the analysis. Because the forearm rotation axis is static, we hypothesize that an axis based on bony landmarks is comparable to an axis calculated from dynamic imaging.
Methods
Eight post-mortem human forearms were scanned using CT in seven rotational positions from maximum supination to maximum pronation. Three rotation axes were calculated: the landmark, average helical, and circle fit axes. The primary outcome is the difference between the axes expressed as the angle and the minimal distance between them. Secondary outcomes are the orientation errors when modeling pose using the three found axes.
Findings
The mean difference between the landmark and average helical axes was 0.38 degrees and 0.51 mm. The mean difference between the landmark and circle fit axes was 0.40 degrees and 0.51 mm. When modeling the pose of the radius using one of the three axes, the difference between the modeled radius and the scanned radius was in each direction below 2 mm and 1 degree.
Interpretation
The rotation axis of the forearm can be accurately calculated using automatically placed bony landmarks. These findings indicate that determining the forearm rotation axis does not require multiple static images or dynamic imaging. This knowledge should be applied to clinical data to assess its applicability in practice.
使用三维骨模型对前臂旋转进行简单评估
动态医学成像可以确定前臂旋转损伤的原因。然而,它有缺点,这取决于所使用的图像模式,与辐射剂量,需要专门的设备,并在分析中涉及的劳动强度。由于前臂旋转轴是静态的,我们假设基于骨标记的轴与动态成像计算的轴相当。方法对8具尸体前臂进行CT扫描,从最大旋后到最大旋前的7个旋转体位。计算了三个旋转轴:地标轴、平均螺旋轴和圆拟合轴。主要结果是表示为角度的轴与它们之间的最小距离之间的差异。次要结果是使用三个找到的轴建模姿势时的方向误差。结果:标志轴与平均螺旋轴的平均差值分别为0.38°和0.51 mm。地标与圆拟合轴线的平均差值分别为0.40°和0.51 mm。当使用三个轴中的一个对半径的位姿进行建模时,建模半径与扫描半径的差异在每个方向上都小于2mm和1度。前臂的旋转轴可以使用自动放置的骨标记精确计算。这些发现表明,确定前臂旋转轴不需要多个静态图像或动态成像。这些知识应应用于临床数据,以评估其在实践中的适用性。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Clinical Biomechanics
医学-工程:生物医学
CiteScore
3.30
自引率
5.60%
发文量
189
审稿时长
12.3 weeks
期刊介绍:
Clinical Biomechanics is an international multidisciplinary journal of biomechanics with a focus on medical and clinical applications of new knowledge in the field.
The science of biomechanics helps explain the causes of cell, tissue, organ and body system disorders, and supports clinicians in the diagnosis, prognosis and evaluation of treatment methods and technologies. Clinical Biomechanics aims to strengthen the links between laboratory and clinic by publishing cutting-edge biomechanics research which helps to explain the causes of injury and disease, and which provides evidence contributing to improved clinical management.
A rigorous peer review system is employed and every attempt is made to process and publish top-quality papers promptly.
Clinical Biomechanics explores all facets of body system, organ, tissue and cell biomechanics, with an emphasis on medical and clinical applications of the basic science aspects. The role of basic science is therefore recognized in a medical or clinical context. The readership of the journal closely reflects its multi-disciplinary contents, being a balance of scientists, engineers and clinicians.
The contents are in the form of research papers, brief reports, review papers and correspondence, whilst special interest issues and supplements are published from time to time.
Disciplines covered include biomechanics and mechanobiology at all scales, bioengineering and use of tissue engineering and biomaterials for clinical applications, biophysics, as well as biomechanical aspects of medical robotics, ergonomics, physical and occupational therapeutics and rehabilitation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


