{"title":"Predicting In-Hospital Mortality in Myocardial Infarction: A Nomogram-Based Retrospective Analysis of the MIMIC-IV Database.","authors":"Shixuan Peng, Qisheng Chen, Weiqi Ke, Yongjun Wu","doi":"10.2147/VHRM.S511277","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite significant advancements in early reperfusion therapy and pharmacological treatment, which have reduced mortality rates after myocardial infarction in recent decades, the in-hospital mortality rate remains high due to factors such as rapid disease progression, comorbid conditions, and potential complications. We aimed to develop and validate a predictive model for in-hospital mortality in myocardial infarction patients.</p><p><strong>Methods: </strong>LASSO regression analysis, univariate analysis, and multivariate logistic analysis were used to construct the nomogram in the training set, followed by model comparison, internal validation, and sensitivity analysis.</p><p><strong>Results: </strong>The analysis comprised 4688 patients in total. The population of patients was randomly assigned to the training set (n = 3512) and validation set (n = 1176). According to the results of LASSO regression analysis and other results, our nomogram contained a total of 10 independent variables related to patient death, including age, respiratory rate, blood glucose, lactate, PTT, BUN, cerebrovascular disease, chronic lung disease, mild liver disease, and metastatic solid cancer. Moreover, the web calculator and nomogram performed exceptionally well at predicting in-hospital death in myocardial infarction patients. The AUC for the training and validation sets' respective prediction models was 0.869 (95% CI: 0.849-0.889) and 0.846 (95% CI: 0.807-0.875) (<i>p</i><0.01). Compared to the Sequential Organ Failure Assessment (SOFA), the nomogram showed greater discrimination in the training and validation sets, and the calibration plots demonstrated an adequate fit for the nomogram in predicting the risk of in-hospital mortality in both groups. The decision curve analysis (DCA) of the nomogram demonstrated a higher net benefit in the training and validation sets and in terms of clinical usefulness than the SOFA.</p><p><strong>Conclusion: </strong>We developed a useful nomogram model and developed a nomogram-based web calculator to predict in-hospital mortality in myocardial infarction patients, which will support doctors in patient counseling and logical diagnosis and therapy.</p>","PeriodicalId":23597,"journal":{"name":"Vascular Health and Risk Management","volume":"21 ","pages":"461-476"},"PeriodicalIF":2.8000,"publicationDate":"2025-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12169423/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vascular Health and Risk Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/VHRM.S511277","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Despite significant advancements in early reperfusion therapy and pharmacological treatment, which have reduced mortality rates after myocardial infarction in recent decades, the in-hospital mortality rate remains high due to factors such as rapid disease progression, comorbid conditions, and potential complications. We aimed to develop and validate a predictive model for in-hospital mortality in myocardial infarction patients.
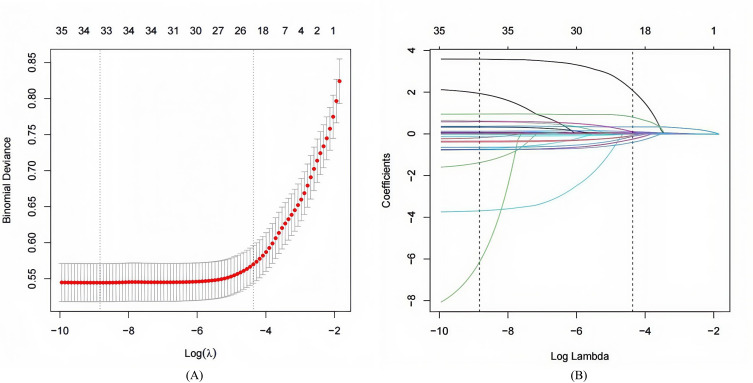
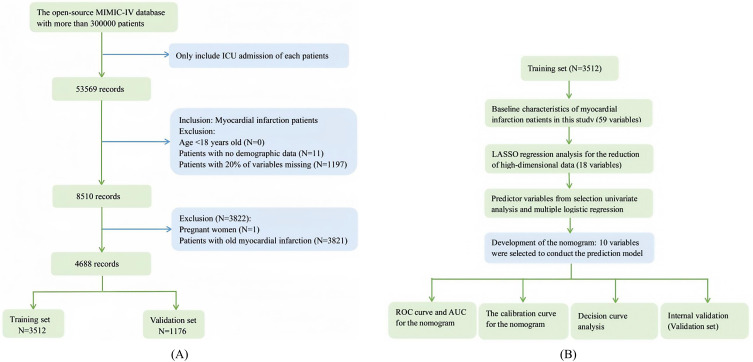
Methods: LASSO regression analysis, univariate analysis, and multivariate logistic analysis were used to construct the nomogram in the training set, followed by model comparison, internal validation, and sensitivity analysis.
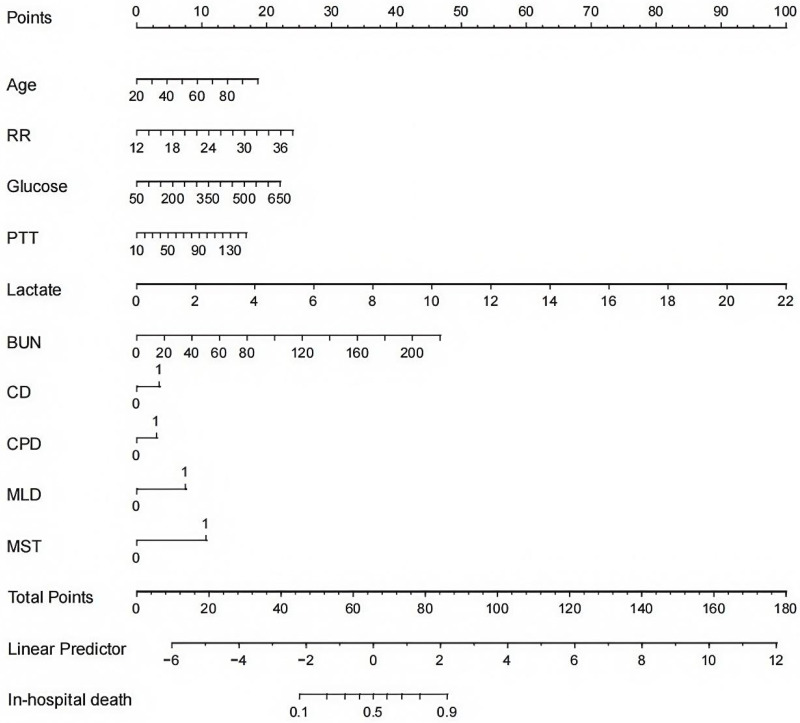
Results: The analysis comprised 4688 patients in total. The population of patients was randomly assigned to the training set (n = 3512) and validation set (n = 1176). According to the results of LASSO regression analysis and other results, our nomogram contained a total of 10 independent variables related to patient death, including age, respiratory rate, blood glucose, lactate, PTT, BUN, cerebrovascular disease, chronic lung disease, mild liver disease, and metastatic solid cancer. Moreover, the web calculator and nomogram performed exceptionally well at predicting in-hospital death in myocardial infarction patients. The AUC for the training and validation sets' respective prediction models was 0.869 (95% CI: 0.849-0.889) and 0.846 (95% CI: 0.807-0.875) (p<0.01). Compared to the Sequential Organ Failure Assessment (SOFA), the nomogram showed greater discrimination in the training and validation sets, and the calibration plots demonstrated an adequate fit for the nomogram in predicting the risk of in-hospital mortality in both groups. The decision curve analysis (DCA) of the nomogram demonstrated a higher net benefit in the training and validation sets and in terms of clinical usefulness than the SOFA.
Conclusion: We developed a useful nomogram model and developed a nomogram-based web calculator to predict in-hospital mortality in myocardial infarction patients, which will support doctors in patient counseling and logical diagnosis and therapy.
期刊介绍:
An international, peer-reviewed journal of therapeutics and risk management, focusing on concise rapid reporting of clinical studies on the processes involved in the maintenance of vascular health; the monitoring, prevention, and treatment of vascular disease and its sequelae; and the involvement of metabolic disorders, particularly diabetes. In addition, the journal will also seek to define drug usage in terms of ultimate uptake and acceptance by the patient and healthcare professional.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


