Jeremy Rosiecki, Natalie Wallace, Katelyn Kammers, Ann-Chee Cheng, Talia Wyckoff, Steven Liu
{"title":"Heavily Pretreated Refractory Diffuse Large B-Cell Lymphoma Successfully Treated with Epcoritamab: Case Report.","authors":"Jeremy Rosiecki, Natalie Wallace, Katelyn Kammers, Ann-Chee Cheng, Talia Wyckoff, Steven Liu","doi":"10.1159/000545372","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Relapsed or refractory diffuse large B-cell lymphoma (DLBCL) poses considerable treatment challenges, with disheartening odds of long-term survival. Numerous strategies exist, including non-cross-resistant combination chemoimmunotherapy regimens, autologous stem cell transplantation, and chimeric antigen receptor (CAR) T-cell therapy, but some patients are not appropriate candidates or cannot sustain response to treatment. Epcoritamab, a bispecific CD20-directed CD3 T-cell engager, has been given accelerated approval by the US Food and Drug Administration for relapsed or refractory DLBCL.</p><p><strong>Case presentation: </strong>We present the case of a 61-year-old male diagnosed with stage 4 \"double-hit\" DLBCL with <i>MYC</i> and <i>BCL6</i> rearrangement, who initially received one cycle of rituximab HyperCVAD (initiated July 23, 2021). He then received dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (DA-EPOCH) followed by high-dose methotrexate and initially responded but relapsed several months later. As the patient was not a candidate for transplant, subsequent treatment rounds included rituximab, gemcitabine, dexamethasone, and cisplatin (R-GDP) and CD19 CAR T-cell therapy; tafasitamab-cxix and lenalidomide; and polatuzumab vedotin plus bendamustine and rituximab (pola-BR). Despite intermittent treatment response, his disease continued to progress. He began treatment with epcoritamab through the early access program but showed early signs of continued progression; his status deteriorated until further treatment had to be withheld. Within approximately 1 month, he could resume treatment, achieving a Deauville score of 1 approximately 3 months after beginning epcoritamab, and continues follow-up nearly 2 years later.</p><p><strong>Conclusion: </strong>T-cell engager therapies, such as epcoritamab, can play a role in managing patients with refractory DLBCL, including those refractory to CAR T-cell therapy.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"744-750"},"PeriodicalIF":0.7000,"publicationDate":"2025-03-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12169811/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545372","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Relapsed or refractory diffuse large B-cell lymphoma (DLBCL) poses considerable treatment challenges, with disheartening odds of long-term survival. Numerous strategies exist, including non-cross-resistant combination chemoimmunotherapy regimens, autologous stem cell transplantation, and chimeric antigen receptor (CAR) T-cell therapy, but some patients are not appropriate candidates or cannot sustain response to treatment. Epcoritamab, a bispecific CD20-directed CD3 T-cell engager, has been given accelerated approval by the US Food and Drug Administration for relapsed or refractory DLBCL.
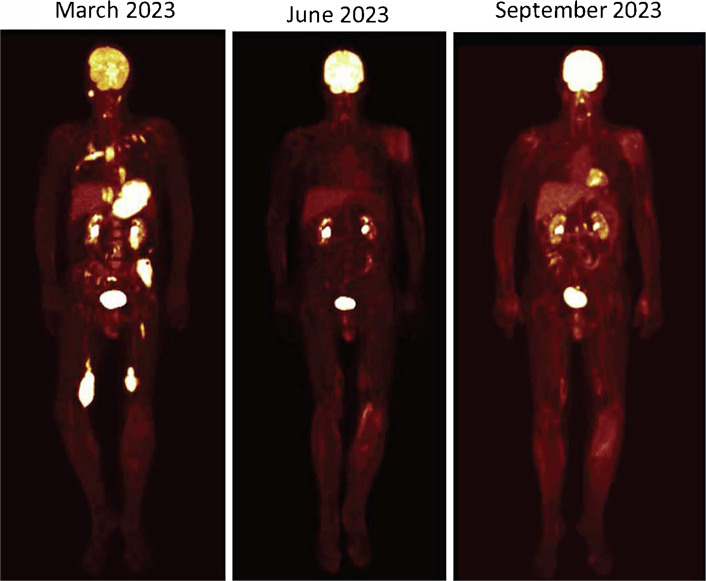
Case presentation: We present the case of a 61-year-old male diagnosed with stage 4 "double-hit" DLBCL with MYC and BCL6 rearrangement, who initially received one cycle of rituximab HyperCVAD (initiated July 23, 2021). He then received dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (DA-EPOCH) followed by high-dose methotrexate and initially responded but relapsed several months later. As the patient was not a candidate for transplant, subsequent treatment rounds included rituximab, gemcitabine, dexamethasone, and cisplatin (R-GDP) and CD19 CAR T-cell therapy; tafasitamab-cxix and lenalidomide; and polatuzumab vedotin plus bendamustine and rituximab (pola-BR). Despite intermittent treatment response, his disease continued to progress. He began treatment with epcoritamab through the early access program but showed early signs of continued progression; his status deteriorated until further treatment had to be withheld. Within approximately 1 month, he could resume treatment, achieving a Deauville score of 1 approximately 3 months after beginning epcoritamab, and continues follow-up nearly 2 years later.
Conclusion: T-cell engager therapies, such as epcoritamab, can play a role in managing patients with refractory DLBCL, including those refractory to CAR T-cell therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


