Claire Claeyssens, Peter Witters, Heidi Segers, Jan De Koster, Elena Levtchenko, Pieter Vermeersch
{"title":"An unusual case of neuroblastoma presenting with prolonged watery diarrhea in a pediatric patient.","authors":"Claire Claeyssens, Peter Witters, Heidi Segers, Jan De Koster, Elena Levtchenko, Pieter Vermeersch","doi":"10.11613/BM.2025.020901","DOIUrl":null,"url":null,"abstract":"<p><p>Neuroblastomas represent a diverse group of neuroblastic tumors characterized by variability in their clinical progression and degree of differentiation. In rare cases, patients with neuroblastoma may present with paraneoplastic syndromes, such as watery diarrhea, hypokalemia, and achlorhydria (WDHA syndrome), linked to the secretion of vasoactive intestinal peptide (VIP). We report a case of a 14-month-old girl presented with a three-week history of watery diarrhea and signs of dehydration with no other symptoms. The patient's medical history was unremarkable, and no medication use was reported. Venous blood gas analysis revealed a normal anion gap metabolic acidosis with severe hypokalemia. The patient was referred to our hospital 48 hours post-admission due to persistent hypokalemic metabolic acidosis, unresponsive to intravenous fluid therapy. The primary causes of normal anion gap metabolic acidosis in young children are gastrointestinal bicarbonate loss due to diarrhea and renal bicarbonate loss. Semi-quantitative urine organic acid analysis, reported 48 hours after admission, revealed increased vanillylmandelic acid (VMA) (89 mmol/mol creatinine) and homovanillic acid (HVA) (21 mmol/mol creatinine), raising the suspicion of a neuroblastoma. Subsequent analysis of an acidified urine sample confirmed a more than threefold increase in VMA, HVA, normetanephrine, norepinephrine, and 3-methoxytyramine concentrations. In addition, VIP was markedly elevated (1994 ng/L) in a blood sample. The diagnosis of neuroblastoma was confirmed through imaging and histological examination. This case illustrates that chronic diarrhea with metabolic dysregulation (<i>e.g.</i> hypokalemia) can be the first and only symptom in patients with VIP-secreting neuroblastoma which can result in delayed diagnosis of neuroblastoma.</p>","PeriodicalId":94370,"journal":{"name":"Biochemia medica","volume":"35 2","pages":"020901"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12161515/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biochemia medica","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.11613/BM.2025.020901","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
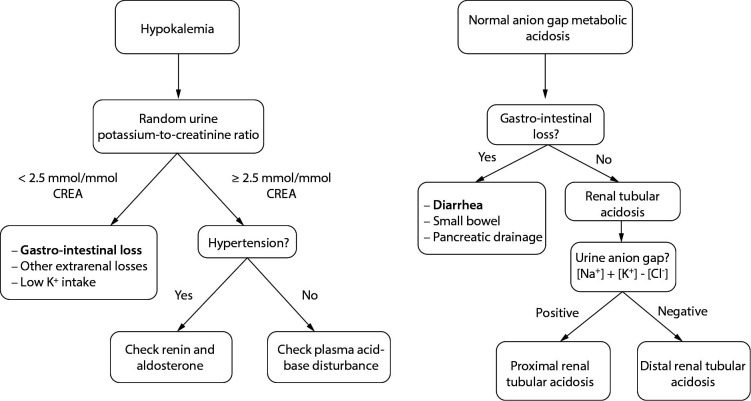
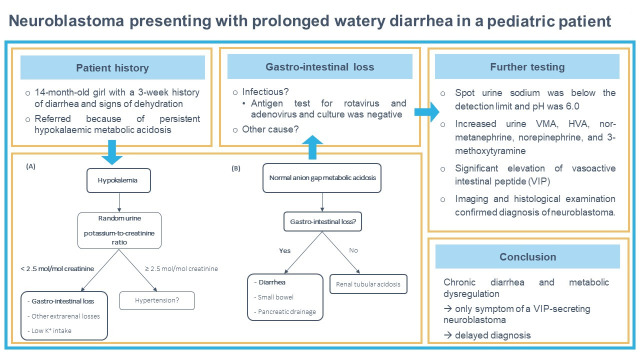
Neuroblastomas represent a diverse group of neuroblastic tumors characterized by variability in their clinical progression and degree of differentiation. In rare cases, patients with neuroblastoma may present with paraneoplastic syndromes, such as watery diarrhea, hypokalemia, and achlorhydria (WDHA syndrome), linked to the secretion of vasoactive intestinal peptide (VIP). We report a case of a 14-month-old girl presented with a three-week history of watery diarrhea and signs of dehydration with no other symptoms. The patient's medical history was unremarkable, and no medication use was reported. Venous blood gas analysis revealed a normal anion gap metabolic acidosis with severe hypokalemia. The patient was referred to our hospital 48 hours post-admission due to persistent hypokalemic metabolic acidosis, unresponsive to intravenous fluid therapy. The primary causes of normal anion gap metabolic acidosis in young children are gastrointestinal bicarbonate loss due to diarrhea and renal bicarbonate loss. Semi-quantitative urine organic acid analysis, reported 48 hours after admission, revealed increased vanillylmandelic acid (VMA) (89 mmol/mol creatinine) and homovanillic acid (HVA) (21 mmol/mol creatinine), raising the suspicion of a neuroblastoma. Subsequent analysis of an acidified urine sample confirmed a more than threefold increase in VMA, HVA, normetanephrine, norepinephrine, and 3-methoxytyramine concentrations. In addition, VIP was markedly elevated (1994 ng/L) in a blood sample. The diagnosis of neuroblastoma was confirmed through imaging and histological examination. This case illustrates that chronic diarrhea with metabolic dysregulation (e.g. hypokalemia) can be the first and only symptom in patients with VIP-secreting neuroblastoma which can result in delayed diagnosis of neuroblastoma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


