{"title":"Evolving roles of systemic therapy in hepatocellular carcinoma: neoadjuvant and adjuvant strategies.","authors":"Ho Soo Chun, Minjong Lee, Tae Hun Kim","doi":"10.17998/jlc.2025.06.13","DOIUrl":null,"url":null,"abstract":"<p><p>Surgical resection for early-stage hepatocellular carcinoma (HCC) provides the potential for long-term survival but recurrence rates within 5 years were up to 70%. Thus, neoadjuvant or adjuvant strategies can be important to improve outcomes. Previous efforts with sorafenib in the adjuvant setting failed to show significant benefits in recurrence-free survival (RFS) or overall survival. However, developments in systemic therapies such as immune checkpoint inhibitors or tyrosine kinase inhibitors have revitalized this field. Although the IMBrave050 trial failed to demonstrate a significant improvement in RFS with one year of adjuvant treatment using atezolizumab combined with bevacizumab in high-risk patients treated with resection or ablation, several other ongoing trials are investigating this promising approach. Neoadjuvant or adjuvant approach using systemic therapies is also gaining attention, supported by phase 1 or 2 clinical trials indicating high objective response rates. In addition, systemic therapies are being increasingly studied as down-staging strategies for resection or liver transplantation. The growing complexity of HCC treatment such as the integration of neoadjuvant and adjuvant strategies underscores the importance of a multidisciplinary approach to optimize therapeutic decision-making in this evolving areas.</p>","PeriodicalId":94087,"journal":{"name":"Journal of liver cancer","volume":" ","pages":"178-186"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12518979/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of liver cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17998/jlc.2025.06.13","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/16 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
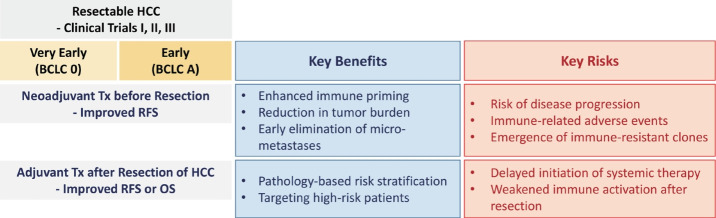
Surgical resection for early-stage hepatocellular carcinoma (HCC) provides the potential for long-term survival but recurrence rates within 5 years were up to 70%. Thus, neoadjuvant or adjuvant strategies can be important to improve outcomes. Previous efforts with sorafenib in the adjuvant setting failed to show significant benefits in recurrence-free survival (RFS) or overall survival. However, developments in systemic therapies such as immune checkpoint inhibitors or tyrosine kinase inhibitors have revitalized this field. Although the IMBrave050 trial failed to demonstrate a significant improvement in RFS with one year of adjuvant treatment using atezolizumab combined with bevacizumab in high-risk patients treated with resection or ablation, several other ongoing trials are investigating this promising approach. Neoadjuvant or adjuvant approach using systemic therapies is also gaining attention, supported by phase 1 or 2 clinical trials indicating high objective response rates. In addition, systemic therapies are being increasingly studied as down-staging strategies for resection or liver transplantation. The growing complexity of HCC treatment such as the integration of neoadjuvant and adjuvant strategies underscores the importance of a multidisciplinary approach to optimize therapeutic decision-making in this evolving areas.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


