Chaoneng Wu, Sujata Kambhatla, Andrew Zazaian, Ali Jaber, Barry Brenner, Chadi Saad
{"title":"Pleiotropic Effects of Cocaine Abuse in Hyperglycemic Crisis: Main Culprit or Accomplice but Never an Innocent Bystander.","authors":"Chaoneng Wu, Sujata Kambhatla, Andrew Zazaian, Ali Jaber, Barry Brenner, Chadi Saad","doi":"10.1177/11795514251341383","DOIUrl":null,"url":null,"abstract":"<p><p>Hyperglycemic crises, including diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state (HHS), significantly affect clinical outcomes and impose a heavy economic burden. Among the steadily increased recreational drug abuse, cocaine has become the most frequently misused substance. However, there is limited understanding of the relationship between cocaine use and hyperglycemic crises. We report 4 cases retrospectively to examine the relationship between cocaine abuse and DKA/HHS. In Case 1, a patient with Type 1 diabetes mellitus (T1DM) presented with altered mental status and a combination of DKA and HHS, where cocaine use led to missed insulin doses, resulting in the crisis. Case 2 involved the same patient who later developed DKA due to cavitary pneumonia and sepsis, requiring mechanical ventilation, vasopressors, and renal replacement therapy. Cocaine inhalation caused pulmonary damage that triggered DKA. Case 3 involved a patient with Type 2 diabetes mellitus (T2DM) who abused cocaine intravenously, leading to DKA-HHS and necrotizing fasciitis that required emergency surgery. Case 4 was a patient with obesity, insulin resistance, and T2DM on oral medications, where cocaine likely exacerbated insulin resistance and triggered DKA. In all 4 cases, treatment focused on aggressive rehydration, insulin infusion, electrolyte correction, and addressing underlying causes. The hyperglycemic crises resolved within 12 to 24 hours. However, managing cocaine-related complications proved difficult, leading to high morbidity and mortality rates, including altered mental status with airway issues, kidney failure, rhabdomyolysis, and infections that could result in septic shock or death. In Case 4, cocaine use significantly worsened insulin resistance and T2DM, contributing to DKA. In conclusion, cocaine abuse has multiple effects and can act as an unusual trigger for hyperglycemic crises by causing missed insulin doses, dehydration, infections, and chronic worsening of insulin resistance. Cocaine abuse can trigger and/or worsen hyperglycemic crises through various mechanisms, such as damage to the cardiopulmonary and renal systems, psychosocial changes, weakened immunity and infections, and alterations in hormones and metabolism (Figure 3). We suggest incorporating questions about substance abuse into routine patient history assessment and performing toxicology screenings, particularly for individuals who have frequent admissions for DKA/HHS. Additionally, we share our expertise in managing this specific group of patients.</p>","PeriodicalId":44715,"journal":{"name":"Clinical Medicine Insights-Endocrinology and Diabetes","volume":"18 ","pages":"11795514251341383"},"PeriodicalIF":3.0000,"publicationDate":"2025-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12166241/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Endocrinology and Diabetes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795514251341383","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
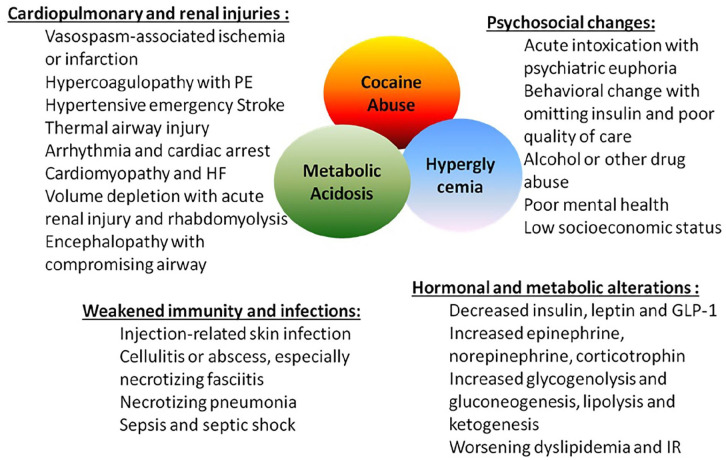
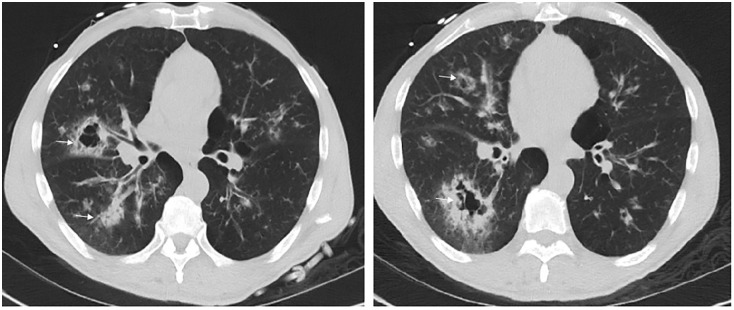
Hyperglycemic crises, including diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state (HHS), significantly affect clinical outcomes and impose a heavy economic burden. Among the steadily increased recreational drug abuse, cocaine has become the most frequently misused substance. However, there is limited understanding of the relationship between cocaine use and hyperglycemic crises. We report 4 cases retrospectively to examine the relationship between cocaine abuse and DKA/HHS. In Case 1, a patient with Type 1 diabetes mellitus (T1DM) presented with altered mental status and a combination of DKA and HHS, where cocaine use led to missed insulin doses, resulting in the crisis. Case 2 involved the same patient who later developed DKA due to cavitary pneumonia and sepsis, requiring mechanical ventilation, vasopressors, and renal replacement therapy. Cocaine inhalation caused pulmonary damage that triggered DKA. Case 3 involved a patient with Type 2 diabetes mellitus (T2DM) who abused cocaine intravenously, leading to DKA-HHS and necrotizing fasciitis that required emergency surgery. Case 4 was a patient with obesity, insulin resistance, and T2DM on oral medications, where cocaine likely exacerbated insulin resistance and triggered DKA. In all 4 cases, treatment focused on aggressive rehydration, insulin infusion, electrolyte correction, and addressing underlying causes. The hyperglycemic crises resolved within 12 to 24 hours. However, managing cocaine-related complications proved difficult, leading to high morbidity and mortality rates, including altered mental status with airway issues, kidney failure, rhabdomyolysis, and infections that could result in septic shock or death. In Case 4, cocaine use significantly worsened insulin resistance and T2DM, contributing to DKA. In conclusion, cocaine abuse has multiple effects and can act as an unusual trigger for hyperglycemic crises by causing missed insulin doses, dehydration, infections, and chronic worsening of insulin resistance. Cocaine abuse can trigger and/or worsen hyperglycemic crises through various mechanisms, such as damage to the cardiopulmonary and renal systems, psychosocial changes, weakened immunity and infections, and alterations in hormones and metabolism (Figure 3). We suggest incorporating questions about substance abuse into routine patient history assessment and performing toxicology screenings, particularly for individuals who have frequent admissions for DKA/HHS. Additionally, we share our expertise in managing this specific group of patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


