E Samuel, C Thomas, C Thompson, E Paul, M Cherk, S Ellis, M Siemienowicz, S Tissera, U Samankula, S Scholz, L Zhang, J Grewal, J Cox, C Yu, G Adabi, D Keating, J Taverner, J Gooi, S Wayne, J Zalcberg, R G Stirling
{"title":"Optimizing Pre-Operative Clinical Staging in Resectable Non-Small Cell Lung Cancer (NSCLC): A Retrospective Cohort Study.","authors":"E Samuel, C Thomas, C Thompson, E Paul, M Cherk, S Ellis, M Siemienowicz, S Tissera, U Samankula, S Scholz, L Zhang, J Grewal, J Cox, C Yu, G Adabi, D Keating, J Taverner, J Gooi, S Wayne, J Zalcberg, R G Stirling","doi":"10.1111/1759-7714.70108","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurate pre-operative clinical staging is essential for guiding treatment in resectable non-small cell lung cancer (NSCLC). Discrepancies between clinical and pathological staging raise concerns about treatment appropriateness. This study aimed to assess staging accuracy, identify predictors of discordance, and evaluate survival implications.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of Stage I-IIIA NSCLC patients who underwent surgical resection in Melbourne, Australia, between 2011 and 2020. Clinical staging was based on CT, PET, and nodal evaluation; pathological staging was based on surgical histology. The primary outcome was concordance between clinical (cTN) and pathological (pTN) stage. Multivariable logistic and Cox regression models evaluated predictors of discordance and survival.</p><p><strong>Results: </strong>Among 221 patients, 58% had concordant clinical and pathological staging. Discordance occurred in 42% of cases-23.9% were upstaged and 17.2% downstaged. N-stage concordance was associated with female sex, tumor histology, SUV max, and CT-to-surgery interval. Nodal discordance independently predicted worse survival (HR 0.43, 95% CI: 0.24-0.77; p = 0.01).</p><p><strong>Conclusions: </strong>Substantial discrepancies exist between clinical and pathological staging in resectable NSCLC. Nodal stage discordance is an independent predictor of mortality and highlights the need for improved pre-operative staging strategies to ensure guideline-concordant care.</p>","PeriodicalId":23338,"journal":{"name":"Thoracic Cancer","volume":"16 11","pages":"e70108"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12168232/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/1759-7714.70108","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
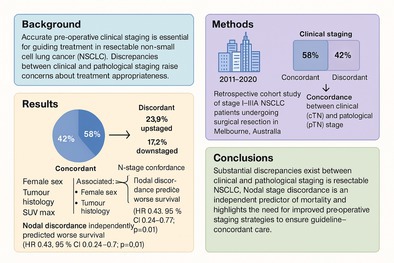
Background: Accurate pre-operative clinical staging is essential for guiding treatment in resectable non-small cell lung cancer (NSCLC). Discrepancies between clinical and pathological staging raise concerns about treatment appropriateness. This study aimed to assess staging accuracy, identify predictors of discordance, and evaluate survival implications.
Methods: We conducted a retrospective cohort study of Stage I-IIIA NSCLC patients who underwent surgical resection in Melbourne, Australia, between 2011 and 2020. Clinical staging was based on CT, PET, and nodal evaluation; pathological staging was based on surgical histology. The primary outcome was concordance between clinical (cTN) and pathological (pTN) stage. Multivariable logistic and Cox regression models evaluated predictors of discordance and survival.
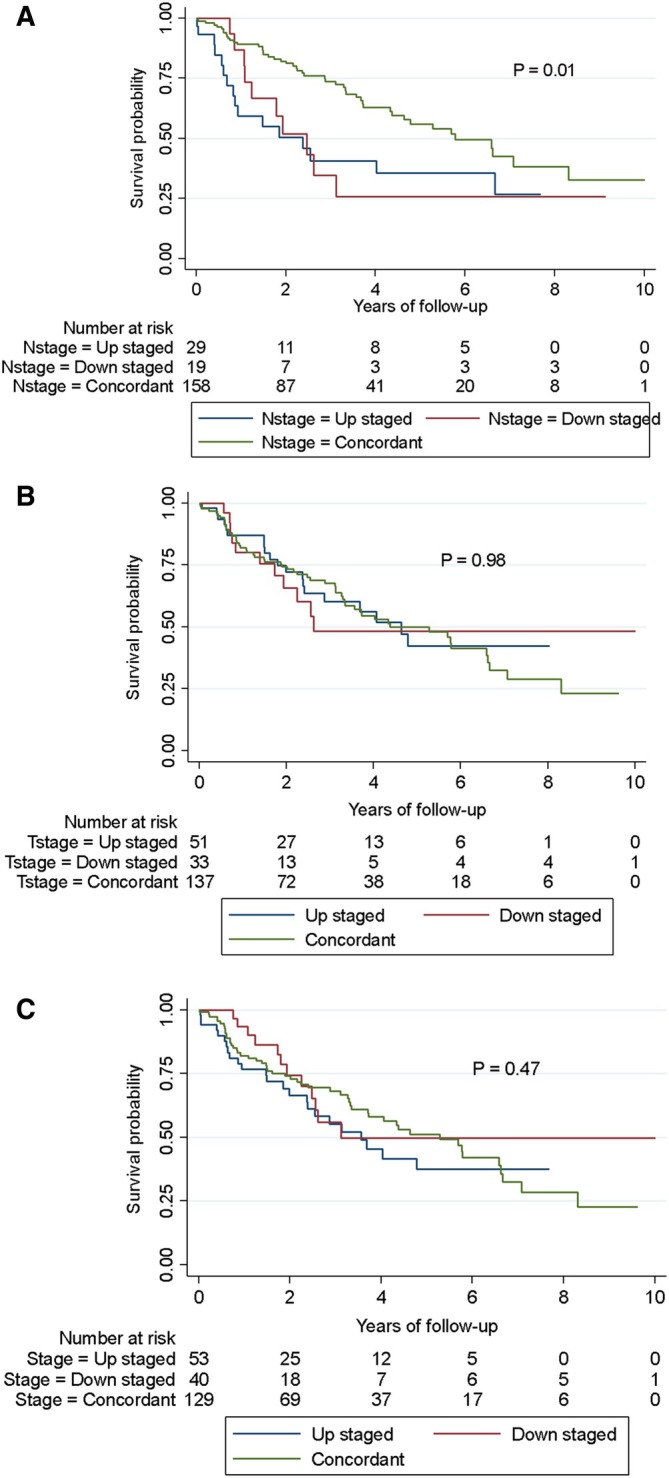
Results: Among 221 patients, 58% had concordant clinical and pathological staging. Discordance occurred in 42% of cases-23.9% were upstaged and 17.2% downstaged. N-stage concordance was associated with female sex, tumor histology, SUV max, and CT-to-surgery interval. Nodal discordance independently predicted worse survival (HR 0.43, 95% CI: 0.24-0.77; p = 0.01).
Conclusions: Substantial discrepancies exist between clinical and pathological staging in resectable NSCLC. Nodal stage discordance is an independent predictor of mortality and highlights the need for improved pre-operative staging strategies to ensure guideline-concordant care.
期刊介绍:
Thoracic Cancer aims to facilitate international collaboration and exchange of comprehensive and cutting-edge information on basic, translational, and applied clinical research in lung cancer, esophageal cancer, mediastinal cancer, breast cancer and other thoracic malignancies. Prevention, treatment and research relevant to Asia-Pacific is a focus area, but submissions from all regions are welcomed. The editors encourage contributions relevant to prevention, general thoracic surgery, medical oncology, radiology, radiation medicine, pathology, basic cancer research, as well as epidemiological and translational studies in thoracic cancer. Thoracic Cancer is the official publication of the Chinese Society of Lung Cancer, International Chinese Society of Thoracic Surgery and is endorsed by the Korean Association for the Study of Lung Cancer and the Hong Kong Cancer Therapy Society.
The Journal publishes a range of article types including: Editorials, Invited Reviews, Mini Reviews, Original Articles, Clinical Guidelines, Technological Notes, Imaging in thoracic cancer, Meeting Reports, Case Reports, Letters to the Editor, Commentaries, and Brief Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


