{"title":"Successful Prevention of Bronchopleural Fistula in Single-Stage Esophagectomy and Right Lower Lobectomy: A Case Report.","authors":"Tomonari Oki, Shuhei Iizuka, Makoto Tomatsu, Toru Nakamura","doi":"10.70352/scrj.cr.25-0170","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Bronchopleural fistulae (BPFs) following pulmonary resection are potentially fatal complications, with right lower lobectomy being the most susceptible among lobectomies. As esophagectomy also increases the risk of tracheobronchial ischemia and postoperative malnutrition, performing a single-stage esophagectomy combined with right lower lobectomy may further elevate the risk of BPFs, underscoring the need for meticulous preoperative planning.</p><p><strong>Case presentation: </strong>A 64-year-old male with a history of heavy smoking was referred to our hospital after an abnormal mass was detected on a chest radiograph during an annual health check. Chest CT revealed a 3.7 cm consolidative mass in the right lower lobe, resulting in a diagnosis of primary lung cancer, classified as T2aN0M0, stage IB. Additionally, abnormal fluorodeoxyglucose (FDG) uptake was observed in the lower thoracic esophagus, leading to a diagnosis of synchronous esophageal cancer, classified as T1bN0M0, stage I. As both lesions required upfront surgical resection via the right thoracic cavity, a single-stage esophagectomy and right lower lobectomy were planned. Initially, esophagectomy was performed using a five-port video-assisted thoracic surgery (VATS) approach in the prone position from the right side. To preserve the blood supply to the fifth intercostal muscle for subsequent harvesting as a muscle flap, the utility port in the corresponding intercostal space was placed as ventrally as possible. The esophagectomy was performed while preserving the right main bronchial artery. The patient was then repositioned to the left lateral decubitus position, and the preserved fifth intercostal muscle flap was harvested. A right lower lobectomy was completed, preserving the bronchial artery, and the bronchial stump was reinforced using the harvested muscle flap. Despite postoperative development of esophagogastric anastomotic leakage, the patient did not develop a BPF, and no signs of BPF have been observed during 12 months of follow-up.</p><p><strong>Conclusions: </strong>Preservation of the right main bronchial artery and reinforcement of the bronchial stump with an intercostal muscle flap facilitated prevention of BPF following single-stage esophagectomy and right lower lobectomy, despite the patient's history of heavy smoking and transient postoperative malnutrition.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12162247/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0170","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/11 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Bronchopleural fistulae (BPFs) following pulmonary resection are potentially fatal complications, with right lower lobectomy being the most susceptible among lobectomies. As esophagectomy also increases the risk of tracheobronchial ischemia and postoperative malnutrition, performing a single-stage esophagectomy combined with right lower lobectomy may further elevate the risk of BPFs, underscoring the need for meticulous preoperative planning.
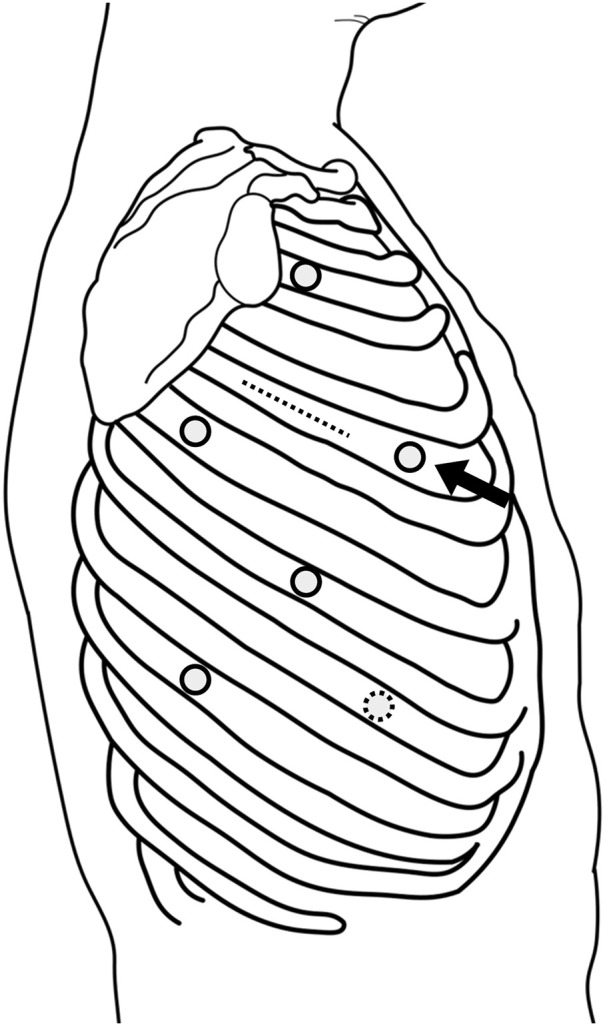
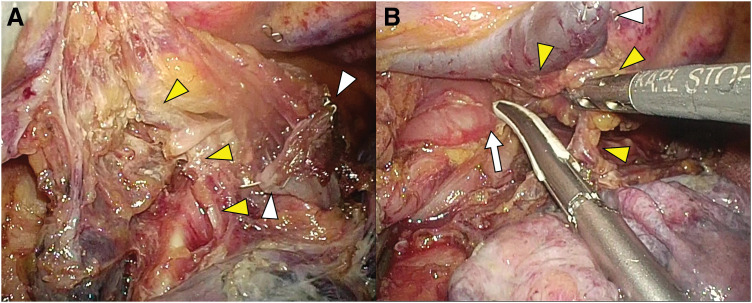
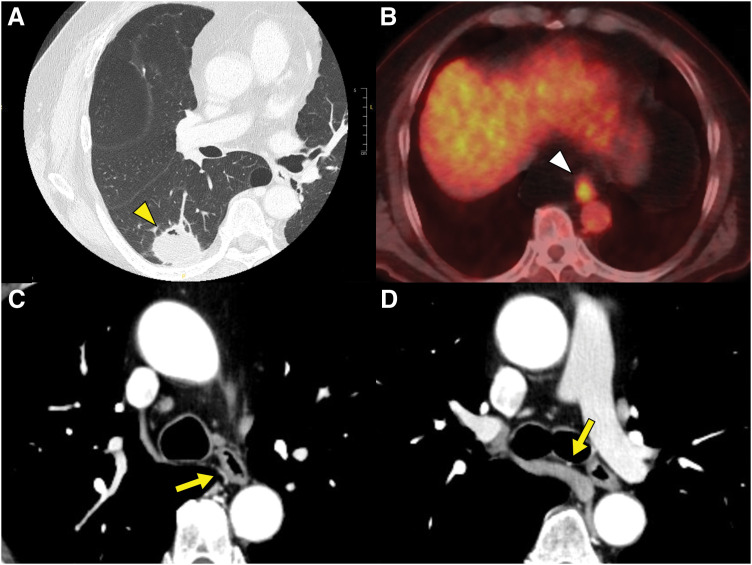
Case presentation: A 64-year-old male with a history of heavy smoking was referred to our hospital after an abnormal mass was detected on a chest radiograph during an annual health check. Chest CT revealed a 3.7 cm consolidative mass in the right lower lobe, resulting in a diagnosis of primary lung cancer, classified as T2aN0M0, stage IB. Additionally, abnormal fluorodeoxyglucose (FDG) uptake was observed in the lower thoracic esophagus, leading to a diagnosis of synchronous esophageal cancer, classified as T1bN0M0, stage I. As both lesions required upfront surgical resection via the right thoracic cavity, a single-stage esophagectomy and right lower lobectomy were planned. Initially, esophagectomy was performed using a five-port video-assisted thoracic surgery (VATS) approach in the prone position from the right side. To preserve the blood supply to the fifth intercostal muscle for subsequent harvesting as a muscle flap, the utility port in the corresponding intercostal space was placed as ventrally as possible. The esophagectomy was performed while preserving the right main bronchial artery. The patient was then repositioned to the left lateral decubitus position, and the preserved fifth intercostal muscle flap was harvested. A right lower lobectomy was completed, preserving the bronchial artery, and the bronchial stump was reinforced using the harvested muscle flap. Despite postoperative development of esophagogastric anastomotic leakage, the patient did not develop a BPF, and no signs of BPF have been observed during 12 months of follow-up.
Conclusions: Preservation of the right main bronchial artery and reinforcement of the bronchial stump with an intercostal muscle flap facilitated prevention of BPF following single-stage esophagectomy and right lower lobectomy, despite the patient's history of heavy smoking and transient postoperative malnutrition.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


