Fei Xiang, Lin Chen, Eric E Roselli, Brian Griffin, Milind Desai, Jeevanantham Rajeswaran, Austin Firth, Eugene H Blackstone, Lars G Svensson
{"title":"Root Remodeling versus Root Reimplantation in Patients with Bicuspid Aortic Valve and Root Aneurysm.","authors":"Fei Xiang, Lin Chen, Eric E Roselli, Brian Griffin, Milind Desai, Jeevanantham Rajeswaran, Austin Firth, Eugene H Blackstone, Lars G Svensson","doi":"10.1055/s-0045-1809688","DOIUrl":null,"url":null,"abstract":"<p><p>Valve-sparing root replacements are increasingly being performed in patients with bicuspid aortic valve (BAV) and root aneurysm. This study aims to compare the outcomes of patients who underwent root remodeling versus root reimplantation.From 2000 to 2022, 206 adults with BAV and root aneurysm (mean age: 47 ± 12 years, 183 [89%] male) underwent root remodeling (<i>n</i> = 32) or reimplantation (<i>n</i> = 174) at Cleveland Clinic. Compared with remodeling, patients in the reimplantation group had more aortic regurgitation (severe 61/174 [35%] vs. 3/32 [9.4%]) and smaller aortic roots (sinus diameter: 4.3 ± 0.56 vs. 4.6 ± 0.47 cm). Operative mortality and morbidity, durability, and time-related mortality were compared.Patients in both groups underwent additional aortic valve repair (reimplantation vs. remodeling group: figure-of-8 hitch-up stitch 10/174 [5.7%] vs. 14/32 [44%], <i>p</i> < 0.001; cusp plication 91/174 [52%] vs. 11/32 [34%], <i>p</i> = 0.06). Compared with the remodeling group, aortic clamp time was longer in the reimplantation group (median 136 vs. 76 minutes, <i>p</i> < 0.001). Two in-hospital reoperations occurred after remodeling from valve dysfunction. One operative death occurred in each group. At 5 years, severe aortic regurgitation was 16% after remodeling versus 5.0% after reimplantation (<i>p</i> = 0.06), mean gradient 11 versus 10 mm Hg (<i>p</i> = 0.12), aortic valve reoperation 23% versus 6.0% (<i>p</i> = 0.14), and survival 97% versus 95%, respectively (<i>p</i> = 0.71).Both root remodeling and reimplantation can be safely performed in patients with BAV and root aneurysms with similar midterm outcomes. Although root remodeling is a shorter surgery, less late aortic valve regurgitation and fewer valve reoperations lead us to recommend root reimplantation.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"1-8"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202024/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1809688","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
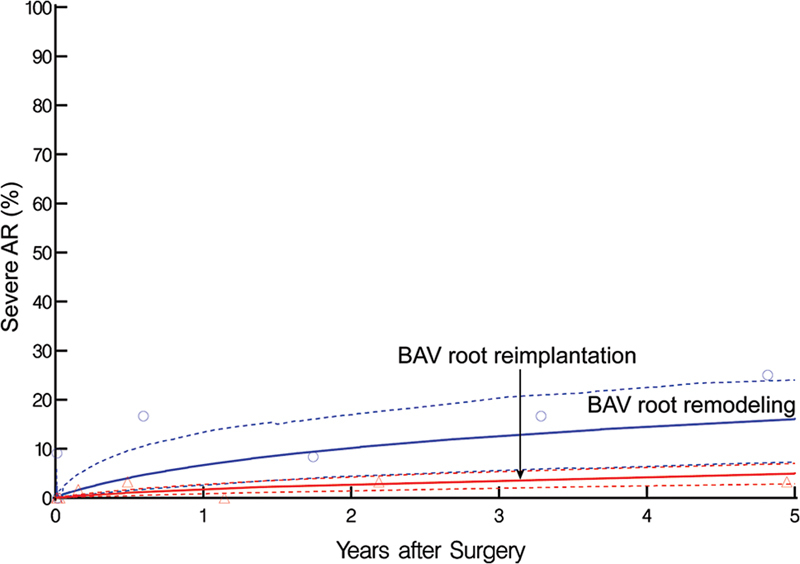
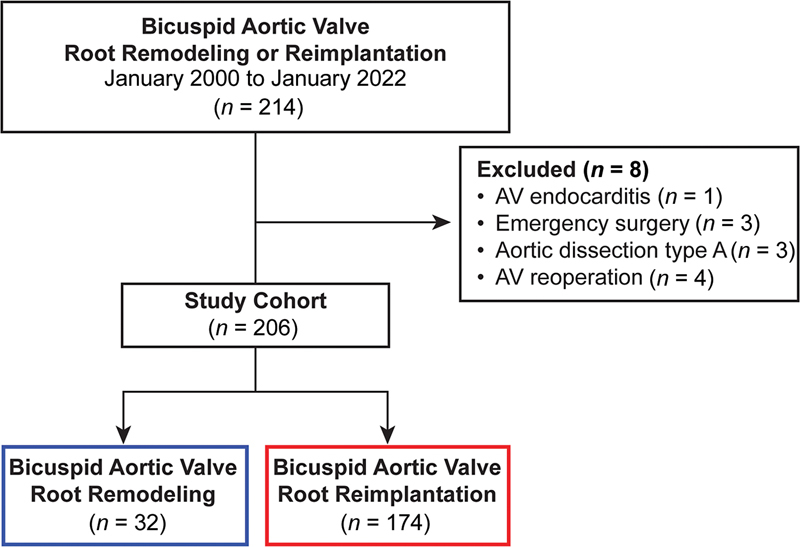
Valve-sparing root replacements are increasingly being performed in patients with bicuspid aortic valve (BAV) and root aneurysm. This study aims to compare the outcomes of patients who underwent root remodeling versus root reimplantation.From 2000 to 2022, 206 adults with BAV and root aneurysm (mean age: 47 ± 12 years, 183 [89%] male) underwent root remodeling (n = 32) or reimplantation (n = 174) at Cleveland Clinic. Compared with remodeling, patients in the reimplantation group had more aortic regurgitation (severe 61/174 [35%] vs. 3/32 [9.4%]) and smaller aortic roots (sinus diameter: 4.3 ± 0.56 vs. 4.6 ± 0.47 cm). Operative mortality and morbidity, durability, and time-related mortality were compared.Patients in both groups underwent additional aortic valve repair (reimplantation vs. remodeling group: figure-of-8 hitch-up stitch 10/174 [5.7%] vs. 14/32 [44%], p < 0.001; cusp plication 91/174 [52%] vs. 11/32 [34%], p = 0.06). Compared with the remodeling group, aortic clamp time was longer in the reimplantation group (median 136 vs. 76 minutes, p < 0.001). Two in-hospital reoperations occurred after remodeling from valve dysfunction. One operative death occurred in each group. At 5 years, severe aortic regurgitation was 16% after remodeling versus 5.0% after reimplantation (p = 0.06), mean gradient 11 versus 10 mm Hg (p = 0.12), aortic valve reoperation 23% versus 6.0% (p = 0.14), and survival 97% versus 95%, respectively (p = 0.71).Both root remodeling and reimplantation can be safely performed in patients with BAV and root aneurysms with similar midterm outcomes. Although root remodeling is a shorter surgery, less late aortic valve regurgitation and fewer valve reoperations lead us to recommend root reimplantation.
保留瓣膜的根置换术越来越多地用于双尖瓣主动脉瓣(BAV)和根动脉瘤患者。本研究的目的是比较患者进行根重塑和根再植的结果。从2000年到2022年,206名成人BAV和根动脉瘤患者(平均年龄:47±12岁,183名[89%]男性)在克利夫兰诊所接受了根重塑(n = 32)或再植(n = 174)。与重构组相比,再植入术组患者主动脉反流较多(严重61/174 [35%]vs. 3/32[9.4%]),主动脉根较小(窦径:4.3±0.56 vs. 4.6±0.47 cm)。比较手术死亡率、发病率、持续时间和与时间相关的死亡率。两组患者均接受了额外的主动脉瓣修复(再植组与重塑组:8字形悬吊缝线10/174 [5.7%]vs. 14/32 [44%], p p = 0.06)。与重构组相比,再植入术组主动脉夹持时间更长(中位136分钟vs. 76分钟,p p = 0.06),平均梯度11 vs. 10 mm Hg (p = 0.12),主动脉瓣再手术23% vs. 6.0% (p = 0.14),生存率分别为97% vs. 95% (p = 0.71)。对于中期预后相似的BAV和根动脉瘤患者,根重构和再植入术都是安全的。虽然根重塑是一个较短的手术,但较少的晚期主动脉瓣反流和瓣膜再手术使我们推荐根再植。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


