Real-life utilization of sentinel lymph node mapping in endometrial cancer: Patterns of practice in unmapped patients and effect on treatment and outcomes.
Danielle Glassman, Raadhika Kher, Cande V Ananth, Eugenia Girda
{"title":"Real-life utilization of sentinel lymph node mapping in endometrial cancer: Patterns of practice in unmapped patients and effect on treatment and outcomes.","authors":"Danielle Glassman, Raadhika Kher, Cande V Ananth, Eugenia Girda","doi":"10.1177/20503121251342047","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To examine the real-life utilization of sentinel lymph node mapping for surgical staging of patients with endometrial cancer. We evaluated patterns of surgical staging in unmapped patients and studied how this practice affected adjuvant therapies and survival.</p><p><strong>Methods: </strong>We conducted a retrospective chart review of patients with newly diagnosed endometrial cancer who underwent minimally invasive surgical staging, including sentinel lymph node mapping with cervical injection of indocyanine green from January 2019 to December 2021. Patient demographics, surgical findings, sentinel lymph node mapping, adjuvant therapy, and recurrence rates were collected. Sentinel lymph node detection rates were calculated, and reasons for omitting lymphadenectomy in unmapped patients were evaluated.</p><p><strong>Results: </strong>Among 121 patients, 80 (66%) had successful sentinel lymph node mapping and 41 (34%) failed mapping. Our yearly detection rate was 63%, 68%, and 70% for 2019, 2020, and 2021, respectively. In patients with successful sentinel lymph node mapping, 73.8% were low-grade and 26.2% were high-grade histology. For patients with failed mapping, 75.6% were low-grade and 24.4% were high-grade histology. For the failed mapping cohort, 23 patients (56.1%) had a complete lymphadenectomy performed, of which 3 (13.0%) had positive lymph nodes. Reasons for omitting lymphadenectomy were documented as: (1) intraoperative pathologic evaluation; (2) inability to tolerate Trendelenburg; (3) difficulty with anatomical dissection/visualization; and (4) evidence of locally advanced disease. There were 18 incompletely staged patients, including 8 (44.4%) with low-risk disease, 2 (11.1%) with locally advanced disease, and 1 (5.6%) with serous histology. The remaining 7 (38.9%) unstaged patients were offered and/or received adjuvant radiation based on final pathology. During a short-term follow-up period, no patients in the unmapped or incompletely staged cohorts had a recurrence of the disease.</p><p><strong>Conclusions: </strong>The rate of sentinel lymph node detection is improving. Low-risk disease identified on intraoperative pathology was the most common reason for omitting lymphadenectomy in unmapped patients, and that practice did not seem to affect adjuvant therapy or recurrence of disease.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"13 ","pages":"20503121251342047"},"PeriodicalIF":2.1000,"publicationDate":"2025-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12159469/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121251342047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To examine the real-life utilization of sentinel lymph node mapping for surgical staging of patients with endometrial cancer. We evaluated patterns of surgical staging in unmapped patients and studied how this practice affected adjuvant therapies and survival.
Methods: We conducted a retrospective chart review of patients with newly diagnosed endometrial cancer who underwent minimally invasive surgical staging, including sentinel lymph node mapping with cervical injection of indocyanine green from January 2019 to December 2021. Patient demographics, surgical findings, sentinel lymph node mapping, adjuvant therapy, and recurrence rates were collected. Sentinel lymph node detection rates were calculated, and reasons for omitting lymphadenectomy in unmapped patients were evaluated.
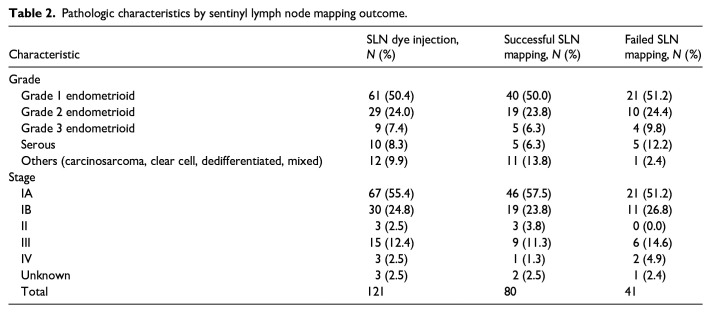
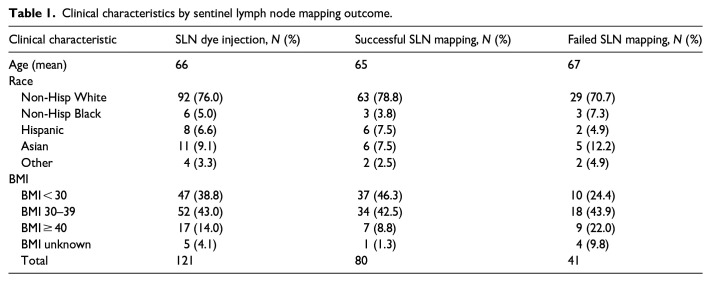
Results: Among 121 patients, 80 (66%) had successful sentinel lymph node mapping and 41 (34%) failed mapping. Our yearly detection rate was 63%, 68%, and 70% for 2019, 2020, and 2021, respectively. In patients with successful sentinel lymph node mapping, 73.8% were low-grade and 26.2% were high-grade histology. For patients with failed mapping, 75.6% were low-grade and 24.4% were high-grade histology. For the failed mapping cohort, 23 patients (56.1%) had a complete lymphadenectomy performed, of which 3 (13.0%) had positive lymph nodes. Reasons for omitting lymphadenectomy were documented as: (1) intraoperative pathologic evaluation; (2) inability to tolerate Trendelenburg; (3) difficulty with anatomical dissection/visualization; and (4) evidence of locally advanced disease. There were 18 incompletely staged patients, including 8 (44.4%) with low-risk disease, 2 (11.1%) with locally advanced disease, and 1 (5.6%) with serous histology. The remaining 7 (38.9%) unstaged patients were offered and/or received adjuvant radiation based on final pathology. During a short-term follow-up period, no patients in the unmapped or incompletely staged cohorts had a recurrence of the disease.
Conclusions: The rate of sentinel lymph node detection is improving. Low-risk disease identified on intraoperative pathology was the most common reason for omitting lymphadenectomy in unmapped patients, and that practice did not seem to affect adjuvant therapy or recurrence of disease.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


