Barry J Plant, Gisli G Einarsson, Kevin F Deasy, Darren Dahly, Pradeep K Singh, Peter J Barry, Christopher H Goss, Isabelle Fajac, Tamara Vagg, Isabelle Durieu, Evelyn Flanagan, Grace O'Callaghan, Clémence Martin, Pierre-Régis Burgel, Charles S Haworth, R Andres Floto, Damian G Downey, Lieven J Dupont, Andrew M Jones, J Stuart Elborn, Joseph A Eustace, Marcus A Mall, Michael M Tunney
{"title":"Cystic Fibrosis Microbiome-directed Antibiotic Therapy Trial in Exacerbations Results Stratified (CFMATTERS): results of a multicentre randomised controlled trial.","authors":"Barry J Plant, Gisli G Einarsson, Kevin F Deasy, Darren Dahly, Pradeep K Singh, Peter J Barry, Christopher H Goss, Isabelle Fajac, Tamara Vagg, Isabelle Durieu, Evelyn Flanagan, Grace O'Callaghan, Clémence Martin, Pierre-Régis Burgel, Charles S Haworth, R Andres Floto, Damian G Downey, Lieven J Dupont, Andrew M Jones, J Stuart Elborn, Joseph A Eustace, Marcus A Mall, Michael M Tunney","doi":"10.1183/13993003.02443-2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study explores the effectiveness and safety of microbiome-directed antimicrobial therapy <i>versus</i> usual antimicrobial therapy in adult cystic fibrosis pulmonary exacerbations.</p><p><strong>Methods: </strong>A multicentre two-arm parallel randomised control trial conducted across Europe/North-America enrolled 223 participants (January 2015 to August 2017). All participants were chronically colonised with <i>Pseudomonas aeruginosa</i> and were randomised 1:1 into two study arms. The \"usual therapy\" group received 2 weeks of intravenous ceftazidime 3 g thrice daily (for allergies: aztreonam 2 g thrice daily) and tobramycin 5-10 mg·kg<sup>-1</sup> once daily. The \"microbiome-directed\" group received the same usual therapy plus an additional antibiotic with greatest presumed activity against the second, third and fourth most abundant genera present in the sputum microbiome, selected by a consensus expert treatment panel. The primary outcome was change in percentage of predicted forced expiratory volume in 1 s (ppFEV<sub>1</sub>) at 14 days post initiation of antibiotics. Secondary outcomes examined ppFEV<sub>1</sub> at 7 days, 28 days and 3 months; time to next exacerbation; symptom burden at 7 days; health-related quality of life (HRQoL) at 28 days; and number of exacerbations and <i>i.v.</i> antibiotic days at 12 months.</p><p><strong>Results: </strong>149 participants had an eligible exacerbation (usual therapy n=83, microbiome-directed therapy n=66). There was no difference between the groups for ppFEV<sub>1</sub> at day 14 (-1.1%, 95% CI -3.9-1.7%; p=0.46), or ppFEV<sub>1</sub> measured at other time points, or for time to next exacerbation (microbiome-directed <i>versus</i> usual therapy hazard ratio 0.91, 95% CI 0.60-1.38; p=0.66). The microbiome-directed group trended to have more <i>i.v.</i> days (median 42 days <i>versus</i> 28 days; p=0.08) and more subsequent exacerbations (median three <i>versus</i> two; p=0.044) the following year. There were no appreciable differences in symptom burden; however, HRQoL subscores were consistently worse in the microbiome-directed group (-4.3 points <i>versus</i> usual therapy, 95% CI -8.3--0.3 points; p=0.033).</p><p><strong>Conclusion: </strong>The addition of a third antibiotic based on sputum microbiome sequencing analysis did not result in improved clinical outcomes.</p>","PeriodicalId":12265,"journal":{"name":"European Respiratory Journal","volume":" ","pages":""},"PeriodicalIF":21.0000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12332466/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Respiratory Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1183/13993003.02443-2024","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"Print","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study explores the effectiveness and safety of microbiome-directed antimicrobial therapy versus usual antimicrobial therapy in adult cystic fibrosis pulmonary exacerbations.
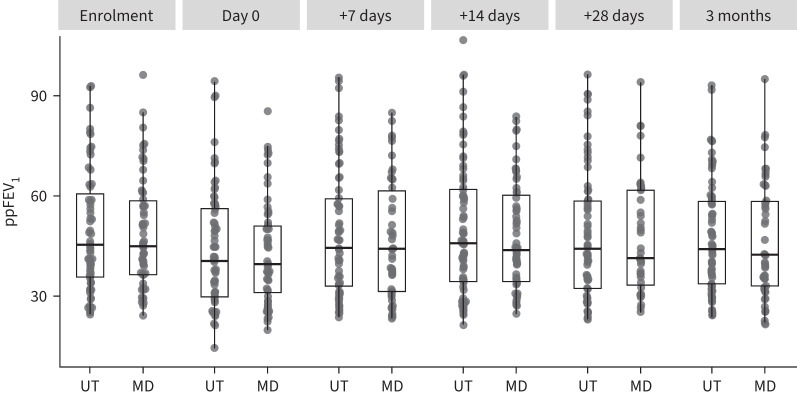
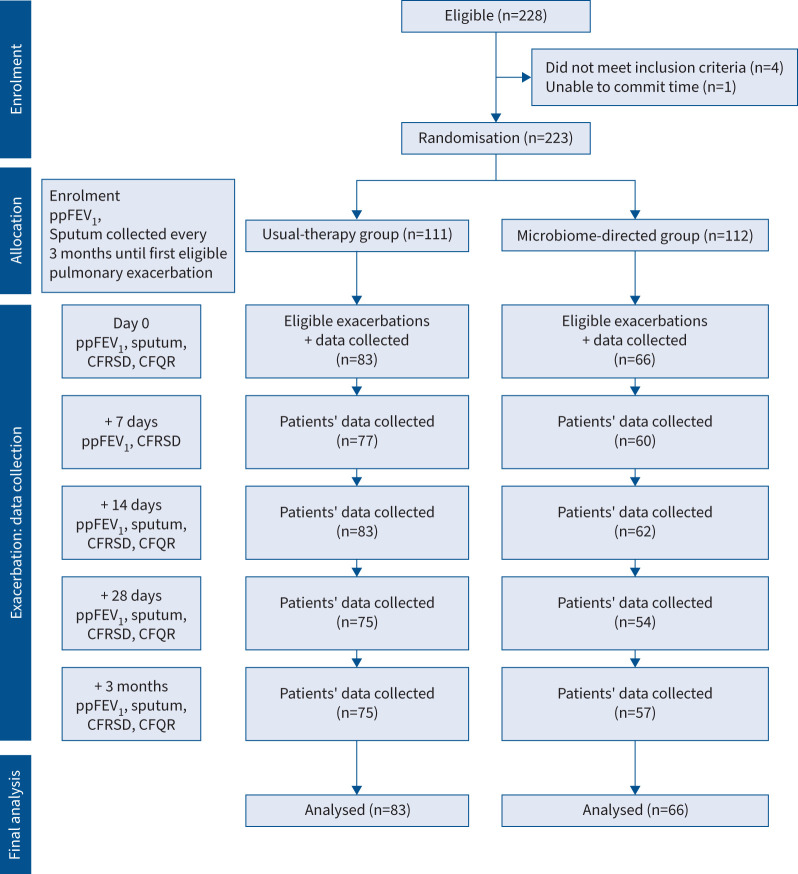
Methods: A multicentre two-arm parallel randomised control trial conducted across Europe/North-America enrolled 223 participants (January 2015 to August 2017). All participants were chronically colonised with Pseudomonas aeruginosa and were randomised 1:1 into two study arms. The "usual therapy" group received 2 weeks of intravenous ceftazidime 3 g thrice daily (for allergies: aztreonam 2 g thrice daily) and tobramycin 5-10 mg·kg-1 once daily. The "microbiome-directed" group received the same usual therapy plus an additional antibiotic with greatest presumed activity against the second, third and fourth most abundant genera present in the sputum microbiome, selected by a consensus expert treatment panel. The primary outcome was change in percentage of predicted forced expiratory volume in 1 s (ppFEV1) at 14 days post initiation of antibiotics. Secondary outcomes examined ppFEV1 at 7 days, 28 days and 3 months; time to next exacerbation; symptom burden at 7 days; health-related quality of life (HRQoL) at 28 days; and number of exacerbations and i.v. antibiotic days at 12 months.
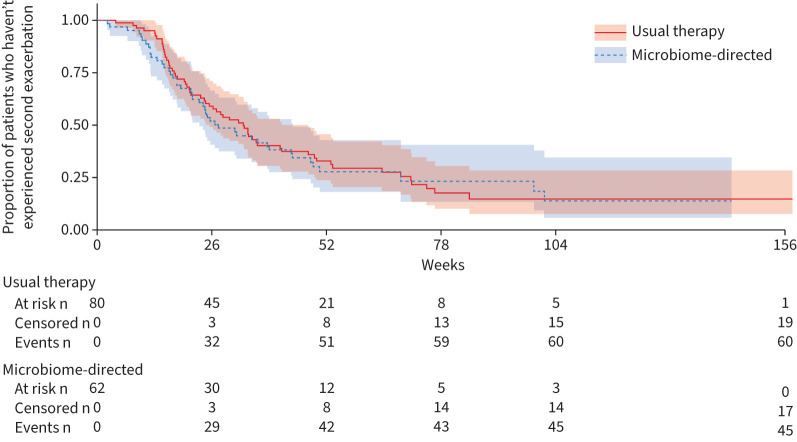
Results: 149 participants had an eligible exacerbation (usual therapy n=83, microbiome-directed therapy n=66). There was no difference between the groups for ppFEV1 at day 14 (-1.1%, 95% CI -3.9-1.7%; p=0.46), or ppFEV1 measured at other time points, or for time to next exacerbation (microbiome-directed versus usual therapy hazard ratio 0.91, 95% CI 0.60-1.38; p=0.66). The microbiome-directed group trended to have more i.v. days (median 42 days versus 28 days; p=0.08) and more subsequent exacerbations (median three versus two; p=0.044) the following year. There were no appreciable differences in symptom burden; however, HRQoL subscores were consistently worse in the microbiome-directed group (-4.3 points versus usual therapy, 95% CI -8.3--0.3 points; p=0.033).
Conclusion: The addition of a third antibiotic based on sputum microbiome sequencing analysis did not result in improved clinical outcomes.
期刊介绍:
The European Respiratory Journal (ERJ) is the flagship journal of the European Respiratory Society. It has a current impact factor of 24.9. The journal covers various aspects of adult and paediatric respiratory medicine, including cell biology, epidemiology, immunology, oncology, pathophysiology, imaging, occupational medicine, intensive care, sleep medicine, and thoracic surgery. In addition to original research material, the ERJ publishes editorial commentaries, reviews, short research letters, and correspondence to the editor. The articles are published continuously and collected into 12 monthly issues in two volumes per year.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


