Ryan G Alexander, John C Cheville, Geoffrey B Thompson, Glenn L Alexander
{"title":"Diarrhea, Weight Loss, and an Elevated Gastrin: A Case Report.","authors":"Ryan G Alexander, John C Cheville, Geoffrey B Thompson, Glenn L Alexander","doi":"10.1159/000545714","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hypergastrinemia in a patient with refractory reflux, steatorrhea, or peptic ulcer disease with a gastric pH <4 is concerning for Zollinger-Ellison syndrome (ZES), but antral G-cell hyperplasia can also present in this manner and is distinguished from ZES based on negative radiographic studies and secretory stimulation testing with a typical gastrin response to a standardized test meal.</p><p><strong>Case presentation: </strong>A 51-year-old female with a history of a Nissen fundoplication for refractory reflux presented with a 3-month history of heartburn, diarrhea, and 55-pound weight loss. Evaluation included negative upper and lower endoscopies with biopsies and negative MR enterography. A 48-h fecal fat study revealed 501 g of stool and 51 g of fat per 24 h. A serum gastrin level off PPI was elevated at 589 pg/mL with a gastric pH of 2 on gastric aspirate. An EUS, DOTATATE PET scan, and secretin stimulation test were negative for ZE. A standardized test meal with serial gastrin monitoring demonstrated an 8-fold increase in serum gastrin. Open abdominal exploration and intraoperative ultrasound showed no evidence of a gastrinoma and an antrectomy and Billroth II anastomosis was performed in treatment of G-cell hyperplasia. Pathology demonstrated a moderately increased G-cell population. Postoperatively, her hypergastrinemia and steatorrhea resolved and she regained 60 pounds.</p><p><strong>Conclusion: </strong>Antral G-cell hyperplasia should be considered in patients with symptoms suggestive of gastrinoma with negative secretin stimulation testing and imaging studies. A standardized test meal demonstrates a substantial increase in serum gastrin levels and antrectomy is the treatment of choice for refractory symptoms.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"428-433"},"PeriodicalIF":0.6000,"publicationDate":"2025-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12158413/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545714","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Hypergastrinemia in a patient with refractory reflux, steatorrhea, or peptic ulcer disease with a gastric pH <4 is concerning for Zollinger-Ellison syndrome (ZES), but antral G-cell hyperplasia can also present in this manner and is distinguished from ZES based on negative radiographic studies and secretory stimulation testing with a typical gastrin response to a standardized test meal.
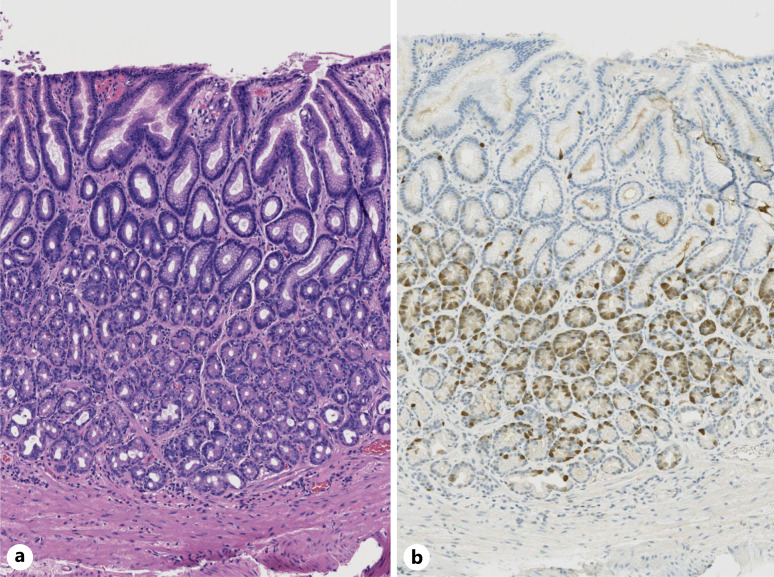
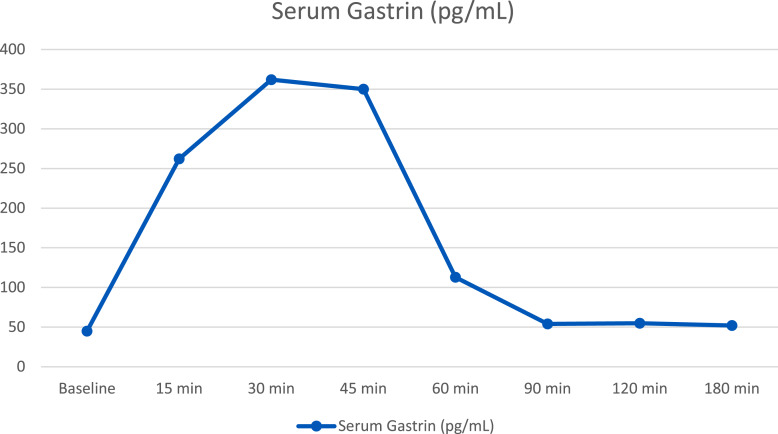
Case presentation: A 51-year-old female with a history of a Nissen fundoplication for refractory reflux presented with a 3-month history of heartburn, diarrhea, and 55-pound weight loss. Evaluation included negative upper and lower endoscopies with biopsies and negative MR enterography. A 48-h fecal fat study revealed 501 g of stool and 51 g of fat per 24 h. A serum gastrin level off PPI was elevated at 589 pg/mL with a gastric pH of 2 on gastric aspirate. An EUS, DOTATATE PET scan, and secretin stimulation test were negative for ZE. A standardized test meal with serial gastrin monitoring demonstrated an 8-fold increase in serum gastrin. Open abdominal exploration and intraoperative ultrasound showed no evidence of a gastrinoma and an antrectomy and Billroth II anastomosis was performed in treatment of G-cell hyperplasia. Pathology demonstrated a moderately increased G-cell population. Postoperatively, her hypergastrinemia and steatorrhea resolved and she regained 60 pounds.
Conclusion: Antral G-cell hyperplasia should be considered in patients with symptoms suggestive of gastrinoma with negative secretin stimulation testing and imaging studies. A standardized test meal demonstrates a substantial increase in serum gastrin levels and antrectomy is the treatment of choice for refractory symptoms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


