Hyun Jeong Jeon, So Jeong Yoon, Ho Chang Chae, Hyeong Seok Kim, Sang Hyun Shin, In Woong Han, Jin Seok Heo, Hongbeom Kim
{"title":"Impact of preoperative prognostic factors on survival outcomes in intrahepatic cholangiocarcinoma: a retrospective cohort study.","authors":"Hyun Jeong Jeon, So Jeong Yoon, Ho Chang Chae, Hyeong Seok Kim, Sang Hyun Shin, In Woong Han, Jin Seok Heo, Hongbeom Kim","doi":"10.4174/astr.2025.108.6.345","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study assesses preoperative prognostic factors in intrahepatic cholangiocarcinoma (ICC) to improve risk assessment and inform clinical decisions, focusing on the role of lymph node dissection (LND).</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 234 patients who underwent surgery for ICC at a single institution between 2010 and 2019. Prognostic factors affecting overall survival (OS) were identified through univariate and multivariable logistic regression analyses. Patients were categorized into high-, intermediate-, and low-risk groups based on the number of adverse prognostic factors. Survival curves were compared between the groups that underwent LND and those that did not within each risk category.</p><p><strong>Results: </strong>Of the 234 patients, 138 (59.0%) underwent LND, and 96 (41.0%) did not (non-LND). Significant prognostic factors included preoperative elevation of CEA (>5 ng/mL), CA 19-9 (>37 U/mL), tumor multiplicity, tumor size >5 cm, and extrahepatic invasion. These factors were associated with adverse OS (hazard ratio ranging from 1.69 to 2.54). High-risk patients had significantly lower median OS compared to intermediate and low-risk groups in both LND and non-LND cohorts, but no significant difference in median OS between LND and non-LND groups within each risk category was observed.</p><p><strong>Conclusion: </strong>Preoperative prognostic factors such as CEA, CA 19-9, tumor size, and multiplicity are vital for assessing patient risk in ICC. These factors guide clinical decision-making and emphasize the need for targeted treatment strategies, including the consideration of LND, particularly in high-risk patients. The study underscores the importance of these prognostic indicators in enhancing treatment outcomes.</p>","PeriodicalId":8071,"journal":{"name":"Annals of Surgical Treatment and Research","volume":"108 6","pages":"345-351"},"PeriodicalIF":1.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149987/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Surgical Treatment and Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4174/astr.2025.108.6.345","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study assesses preoperative prognostic factors in intrahepatic cholangiocarcinoma (ICC) to improve risk assessment and inform clinical decisions, focusing on the role of lymph node dissection (LND).
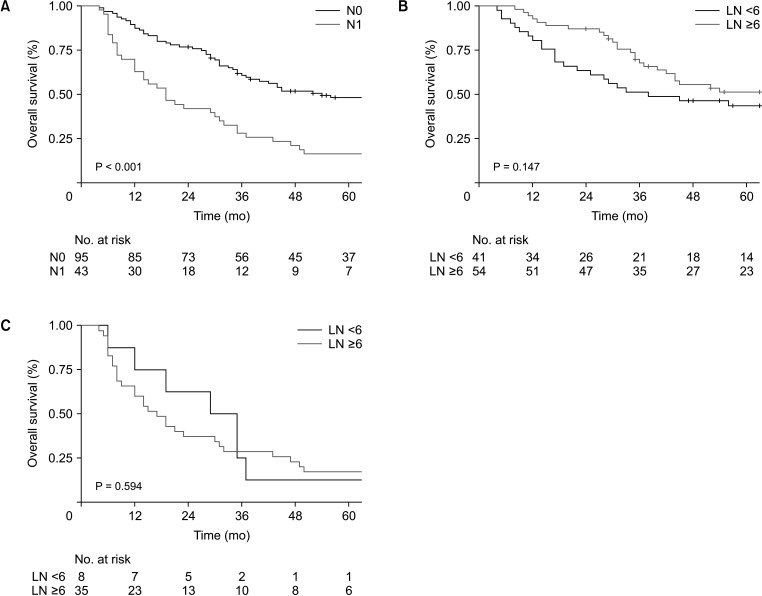
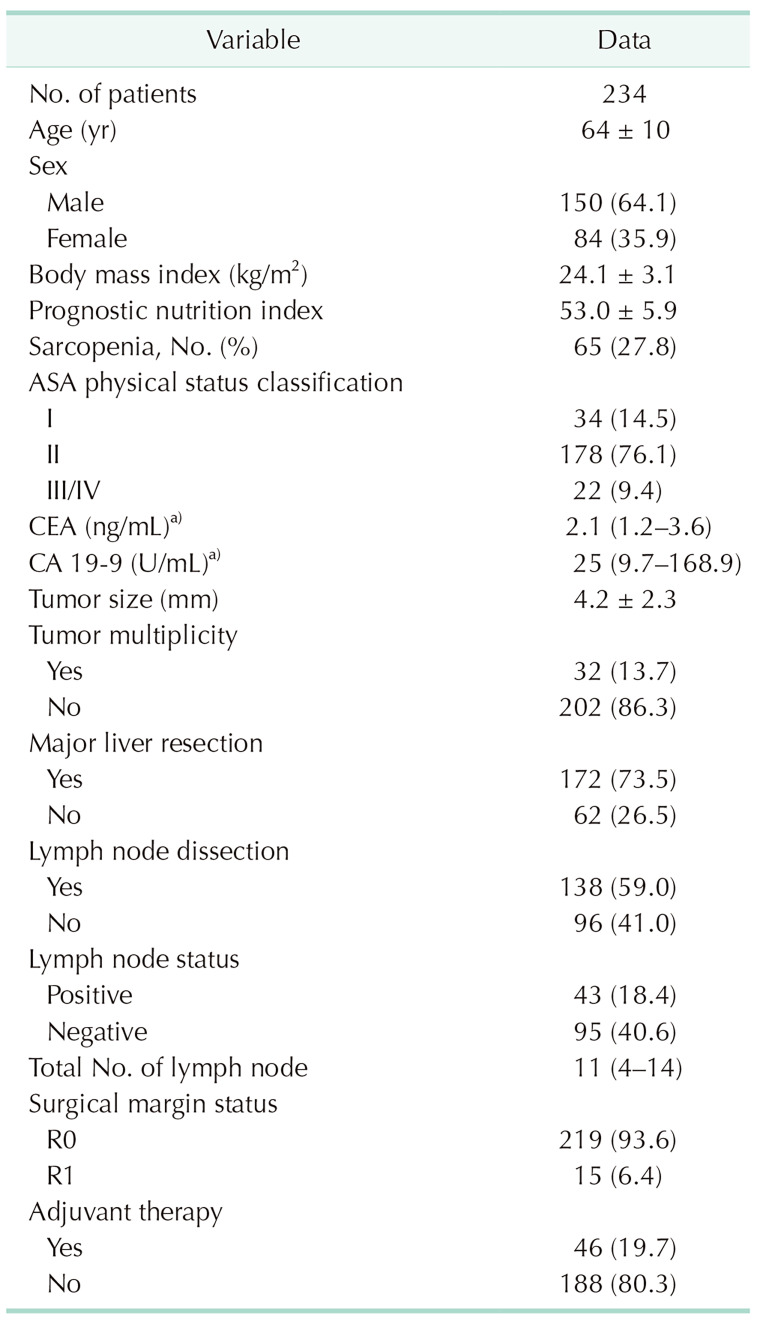
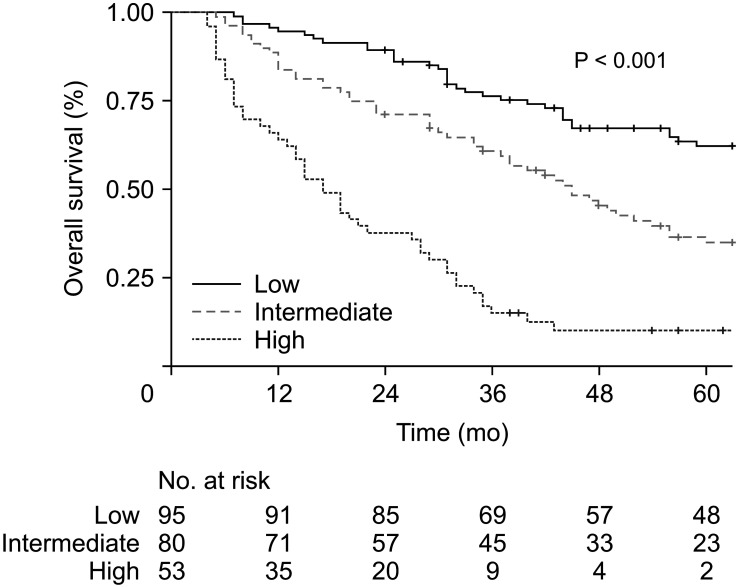
Methods: We conducted a retrospective analysis of 234 patients who underwent surgery for ICC at a single institution between 2010 and 2019. Prognostic factors affecting overall survival (OS) were identified through univariate and multivariable logistic regression analyses. Patients were categorized into high-, intermediate-, and low-risk groups based on the number of adverse prognostic factors. Survival curves were compared between the groups that underwent LND and those that did not within each risk category.
Results: Of the 234 patients, 138 (59.0%) underwent LND, and 96 (41.0%) did not (non-LND). Significant prognostic factors included preoperative elevation of CEA (>5 ng/mL), CA 19-9 (>37 U/mL), tumor multiplicity, tumor size >5 cm, and extrahepatic invasion. These factors were associated with adverse OS (hazard ratio ranging from 1.69 to 2.54). High-risk patients had significantly lower median OS compared to intermediate and low-risk groups in both LND and non-LND cohorts, but no significant difference in median OS between LND and non-LND groups within each risk category was observed.
Conclusion: Preoperative prognostic factors such as CEA, CA 19-9, tumor size, and multiplicity are vital for assessing patient risk in ICC. These factors guide clinical decision-making and emphasize the need for targeted treatment strategies, including the consideration of LND, particularly in high-risk patients. The study underscores the importance of these prognostic indicators in enhancing treatment outcomes.
期刊介绍:
Manuscripts to the Annals of Surgical Treatment and Research (Ann Surg Treat Res) should be written in English according to the instructions for authors. If the details are not described below, the style should follow the Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publications available at International Committee of Medical Journal Editors (ICMJE) website (http://www.icmje.org).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


