{"title":"An Aspirin-Free Strategy for Patients Undergoing Staged Percutaneous Coronary Intervention - A Subgroup Analysis of the STOPDAPT-3 Trial.","authors":"Ko Yamamoto, Masahiro Natsuaki, Hirotoshi Watanabe, Takeshi Morimoto, Yuki Obayashi, Ryusuke Nishikawa, Tomoya Kimura, Kenji Ando, Satoru Suwa, Tsuyoshi Isawa, Hiroyuki Takenaka, Tetsuya Ishikawa, Takafumi Yokomatsu, Toshiya Chinen, Tatsuki Doijiri, Ken Kozuma, Yasunori Nishida, Koji Yamaguchi, Hideki Kitahara, Mitsunori Ishino, Koh Ono, Takeshi Kimura","doi":"10.1253/circrep.CR-25-0026","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>No previous studies have evaluated the effect of an aspirin-free strategy for patients undergoing staged percutaneous coronary intervention (PCI).</p><p><strong>Methods and results: </strong>We conducted a post hoc subgroup analysis in patients undergoing staged PCI within 1 month in STOPDAPT-3 (n=6,002), which randomly compared prasugrel monotherapy with dual antiplatelet therapy (DAPT) in patients with acute coronary syndrome or high bleeding risk. The co-primary endpoints were major bleeding (Bleeding Academic Research Consortium 3 or 5) and cardiovascular events (a composite of cardiovascular death, myocardial infarction, definite stent thrombosis, or stroke) at 1 month. There were 814 patients undergoing staged PCI within 1 month (no-aspirin group, n=401; DAPT group, n=413). The median interval from randomization to the first staged PCI was 8 (interquartile range 5-13) days. More than 90% of the patients received assigned antiplatelet agents at all staged PCI procedures. The effect of no-aspirin relative to DAPT was not different for the co-primary bleeding (3.74% vs. 1.94%; HR 1.94; 95% CI 0.82-4.57) and cardiovascular (3.49% vs. 2.42%; HR 1.44; 95% CI 0.64-3.25) endpoints. The no-aspirin group compared with the DAPT group had a numerically higher incidence of the co-primary cardiovascular endpoint, which occurred after the first staged PCI procedure (2.49% vs. 1.21%; HR 2.07; 95% CI 0.71-6.05).</p><p><strong>Conclusions: </strong>An aspirin-free prasugrel monotherapy relative to DAPT had numerically higher risks of cardiovascular and major bleeding events in patients undergoing staged PCI at 1 month.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 6","pages":"451-462"},"PeriodicalIF":1.1000,"publicationDate":"2025-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12148353/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: No previous studies have evaluated the effect of an aspirin-free strategy for patients undergoing staged percutaneous coronary intervention (PCI).
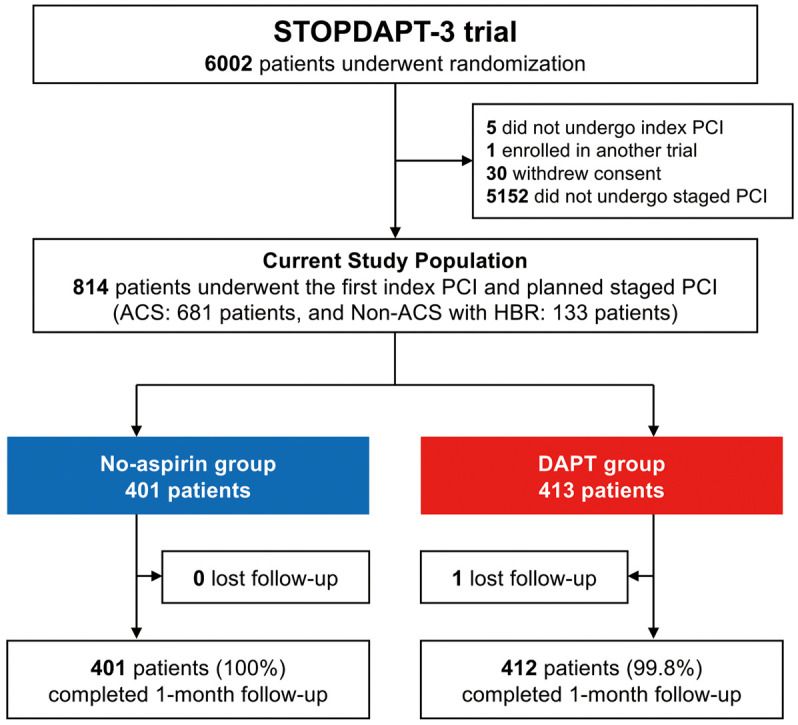
Methods and results: We conducted a post hoc subgroup analysis in patients undergoing staged PCI within 1 month in STOPDAPT-3 (n=6,002), which randomly compared prasugrel monotherapy with dual antiplatelet therapy (DAPT) in patients with acute coronary syndrome or high bleeding risk. The co-primary endpoints were major bleeding (Bleeding Academic Research Consortium 3 or 5) and cardiovascular events (a composite of cardiovascular death, myocardial infarction, definite stent thrombosis, or stroke) at 1 month. There were 814 patients undergoing staged PCI within 1 month (no-aspirin group, n=401; DAPT group, n=413). The median interval from randomization to the first staged PCI was 8 (interquartile range 5-13) days. More than 90% of the patients received assigned antiplatelet agents at all staged PCI procedures. The effect of no-aspirin relative to DAPT was not different for the co-primary bleeding (3.74% vs. 1.94%; HR 1.94; 95% CI 0.82-4.57) and cardiovascular (3.49% vs. 2.42%; HR 1.44; 95% CI 0.64-3.25) endpoints. The no-aspirin group compared with the DAPT group had a numerically higher incidence of the co-primary cardiovascular endpoint, which occurred after the first staged PCI procedure (2.49% vs. 1.21%; HR 2.07; 95% CI 0.71-6.05).
Conclusions: An aspirin-free prasugrel monotherapy relative to DAPT had numerically higher risks of cardiovascular and major bleeding events in patients undergoing staged PCI at 1 month.
背景:以前没有研究评估无阿司匹林策略对分期经皮冠状动脉介入治疗(PCI)患者的影响。方法和结果:我们对1个月内接受stopdpt -3分期PCI治疗的患者(n=6,002)进行了一项事后亚组分析,随机比较了急性冠状动脉综合征或高危出血患者的普拉格雷单药治疗与双重抗血小板治疗(DAPT)。共同主要终点是1个月时的大出血(出血学术研究联盟3或5)和心血管事件(心血管死亡、心肌梗死、明确支架血栓形成或中风的复合)。814例患者在1个月内接受了分期PCI治疗(无阿司匹林组,n=401;DAPT组,n=413)。从随机化到第一阶段PCI的中位时间间隔为8天(四分位数间距为5-13天)。超过90%的患者在所有分期PCI手术中接受了指定的抗血小板药物。对于共同原发性出血,不服用阿司匹林相对于DAPT的效果没有差异(3.74% vs. 1.94%;人力资源1.94;95% CI 0.82-4.57)和心血管(3.49% vs. 2.42%;人力资源1.44;95% CI 0.64-3.25)。与DAPT组相比,无阿司匹林组在第一阶段PCI手术后发生的共同主要心血管终点的发生率更高(2.49% vs. 1.21%;人力资源2.07;95% ci 0.71-6.05)。结论:与DAPT相比,无阿司匹林普拉格雷单药治疗在1个月分期PCI患者中发生心血管和大出血事件的风险更高。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


