{"title":"Myocardial ischemia in nonobstructive coronary arteries: A review of diagnostic dilemmas, current perspectives, and emerging therapeutic innovations.","authors":"Hariharan Seshadri, Dhaiyanitha Gunasekaran, Abdulkader Mohammad, Srinivas Rachoori, Hamrish Kumar Rajakumar","doi":"10.4330/wjc.v17.i5.106541","DOIUrl":null,"url":null,"abstract":"<p><p>Myocardial infarction with nonobstructive coronary arteries is a unique presentation of acute coronary syndrome occurring in patients without significant coronary artery disease. Its pathophysiology involves atherosclerotic and nonatherosclerotic mechanisms such as plaque erosion, coronary microvascular dysfunction, vasospasm, spontaneous coronary artery dissection, autoimmune and inflammatory diseases, and myocardial oxygen supply-demand imbalance. A systematic approach to diagnosis is needed due to the diverse range of underlying causes. Cardiac troponins confirm the myocardial injury and coronary angiography rules out significant obstruction. Cardiac magnetic resonance imaging differentiates ischemic from nonischemic causes, and additional investigations, such as intravascular ultrasound, optical coherence tomography, and provocative testing, play a role in identifying the etiology to guide management strategies. Atherosclerotic cases require antiplatelet therapy and statins, vasospastic cases respond to calcium channel blockers, spontaneous coronary artery dissection is typically managed conservatively, and coronary microvascular dysfunction may require vasodilators. Lifestyle modifications and cardiac rehabilitation are essential for improving outcomes. The prognosis of patients experiencing recurrent events despite treatment is uncertain, but long-term outcomes depend on the etiology, highlighting the need for personalized management. Future research should focus on refining diagnostic protocols and identifying optimal therapeutic strategies. Randomized controlled trials are necessary to establish evidence-based treatments for different subtypes of myocardial infarction with nonobstructive coronary arteries.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 5","pages":"106541"},"PeriodicalIF":2.8000,"publicationDate":"2025-05-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12146959/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i5.106541","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
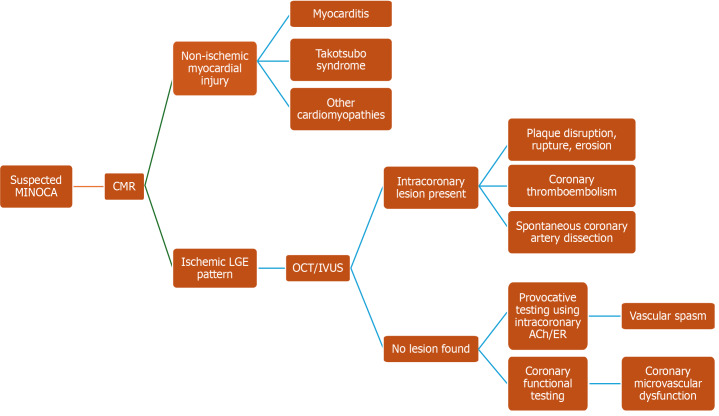
Myocardial infarction with nonobstructive coronary arteries is a unique presentation of acute coronary syndrome occurring in patients without significant coronary artery disease. Its pathophysiology involves atherosclerotic and nonatherosclerotic mechanisms such as plaque erosion, coronary microvascular dysfunction, vasospasm, spontaneous coronary artery dissection, autoimmune and inflammatory diseases, and myocardial oxygen supply-demand imbalance. A systematic approach to diagnosis is needed due to the diverse range of underlying causes. Cardiac troponins confirm the myocardial injury and coronary angiography rules out significant obstruction. Cardiac magnetic resonance imaging differentiates ischemic from nonischemic causes, and additional investigations, such as intravascular ultrasound, optical coherence tomography, and provocative testing, play a role in identifying the etiology to guide management strategies. Atherosclerotic cases require antiplatelet therapy and statins, vasospastic cases respond to calcium channel blockers, spontaneous coronary artery dissection is typically managed conservatively, and coronary microvascular dysfunction may require vasodilators. Lifestyle modifications and cardiac rehabilitation are essential for improving outcomes. The prognosis of patients experiencing recurrent events despite treatment is uncertain, but long-term outcomes depend on the etiology, highlighting the need for personalized management. Future research should focus on refining diagnostic protocols and identifying optimal therapeutic strategies. Randomized controlled trials are necessary to establish evidence-based treatments for different subtypes of myocardial infarction with nonobstructive coronary arteries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


