Sungmin Suh, Sarah Soh, Jong Wook Song, Kim Kwang-Sub, Young-Lan Kwak, Jae-Kwang Shim
{"title":"Association between ex vivo thrombogenicity and ischemic outcome in off-pump coronary surgery.","authors":"Sungmin Suh, Sarah Soh, Jong Wook Song, Kim Kwang-Sub, Young-Lan Kwak, Jae-Kwang Shim","doi":"10.1080/07853890.2025.2514079","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Increased thrombogenicity prohibits favorable ischemic outcomes in coronary artery disease. This study investigated the association between increased maximal amplitude (MA) on thromboelastography (TEG), which reflects high platelet-fibrin clot strength, and 1-year major adverse cardiovascular events (MACE) in patients who underwent isolated multi-vessel off-pump coronary artery bypass surgery (OPCAB).</p><p><strong>Patients and methods: </strong>Data from 657 patients were retrospectively analyzed. TEG was performed post-anesthesia induction. MACE was defined as cardiovascular death, repeat revascularization, myocardial infarction, stroke, or rehospitalization due to heart failure. Patients were analyzed by tertiles of MA (mm). Logistic regression analyzed the association between 1-year MACE and MA.</p><p><strong>Results: </strong>The incidence of MACE increased with MA tertiles (1<sup>st:</sup> [<65.0]: 4.6%; 2<sup>nd</sup> [65.0-70.3]: 9.3%; 3<sup>rd</sup> [≥70.3]: 13%; <i>p</i> = 0.013). Logistic regression adjusted for known risk factors for MACE revealed an increased risk of MACE with higher MA tertiles (odds ratio [OR]: 1.99 [95% confidence interval {CI}: 0.92-4.55], <i>p</i> = 0.089 for the 2<sup>nd</sup> tertile; OR 2.78 [95% CI: 1.32-6.28], <i>p</i> = 0.010 for the 3<sup>rd</sup> tertile). A restricted cubic spline model revealed a linear relationship between MA and 1-year MACE. A 10-mm increase in MA was associated with a two-fold increase in the risk of 1-year MACE. The optimal MA cutoff for predicting MACE was 69.6 (normal range: 50.6-69.4).</p><p><strong>Conclusions: </strong>Increased thrombogenicity, reflected by elevated MA values, was linearly associated with the occurrence of 1-year MACE, highlighting the need for TEG screening and more aggressive, individualized perioperative anticoagulation management in selected patients with increased MA requiring OPCAB.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2514079"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12152992/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2025.2514079","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/10 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Increased thrombogenicity prohibits favorable ischemic outcomes in coronary artery disease. This study investigated the association between increased maximal amplitude (MA) on thromboelastography (TEG), which reflects high platelet-fibrin clot strength, and 1-year major adverse cardiovascular events (MACE) in patients who underwent isolated multi-vessel off-pump coronary artery bypass surgery (OPCAB).
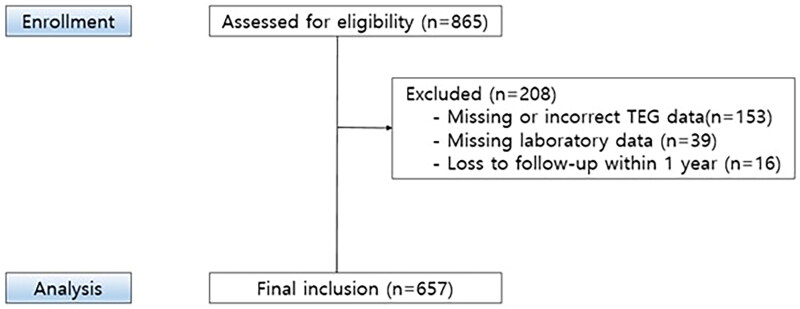
Patients and methods: Data from 657 patients were retrospectively analyzed. TEG was performed post-anesthesia induction. MACE was defined as cardiovascular death, repeat revascularization, myocardial infarction, stroke, or rehospitalization due to heart failure. Patients were analyzed by tertiles of MA (mm). Logistic regression analyzed the association between 1-year MACE and MA.
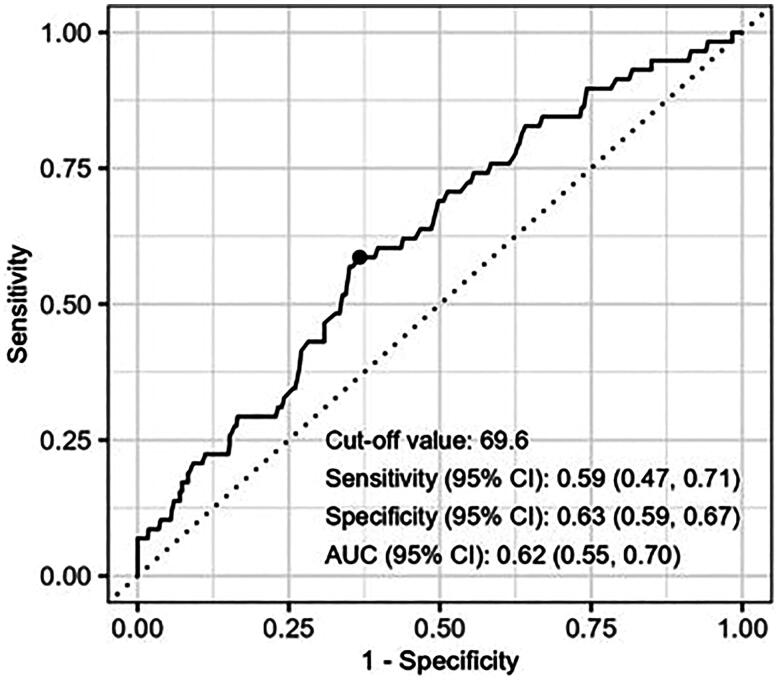
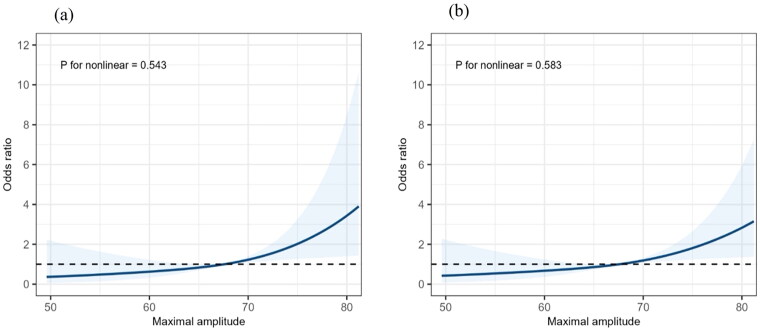
Results: The incidence of MACE increased with MA tertiles (1st: [<65.0]: 4.6%; 2nd [65.0-70.3]: 9.3%; 3rd [≥70.3]: 13%; p = 0.013). Logistic regression adjusted for known risk factors for MACE revealed an increased risk of MACE with higher MA tertiles (odds ratio [OR]: 1.99 [95% confidence interval {CI}: 0.92-4.55], p = 0.089 for the 2nd tertile; OR 2.78 [95% CI: 1.32-6.28], p = 0.010 for the 3rd tertile). A restricted cubic spline model revealed a linear relationship between MA and 1-year MACE. A 10-mm increase in MA was associated with a two-fold increase in the risk of 1-year MACE. The optimal MA cutoff for predicting MACE was 69.6 (normal range: 50.6-69.4).
Conclusions: Increased thrombogenicity, reflected by elevated MA values, was linearly associated with the occurrence of 1-year MACE, highlighting the need for TEG screening and more aggressive, individualized perioperative anticoagulation management in selected patients with increased MA requiring OPCAB.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


