Clara F Weber, Anton Früh, Claudius Jelgersma, Ahmad Almahozi, Kiarash Ferdowssian, Nils Hecht, Peter Vajkoczy, Lars Wessels
{"title":"Systematic review and meta-analysis of spinal versus general anesthesia in decompressive surgeries of the lumbar spine.","authors":"Clara F Weber, Anton Früh, Claudius Jelgersma, Ahmad Almahozi, Kiarash Ferdowssian, Nils Hecht, Peter Vajkoczy, Lars Wessels","doi":"10.1016/j.bas.2025.104280","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Decompressive lumbar spine surgery is a common procedure for disc herniation and spinal stenosis. Besides intervention under general anesthesia (GA), awake surgery (AS) in local or spinal anesthesia offers potential benefits regarding GA-related side effects and simplified periprocedural management.</p><p><strong>Research question: </strong>Within this systematic analysis, we sought to compare postsurgical outcomes of spinal decompression surgeries in GA and AS.</p><p><strong>Methods: </strong>Following the PRISMA guidelines, we extracted all relevant studies from three databases and collected all data concerning surgery duration, blood loss, postoperative duration of hospitalization, postoperative pain (VAS), and disability indices (ODI).</p><p><strong>Results: </strong>In total, we identified 11 studies covering 1350 patients. AS was associated with shorter surgery duration [Mean difference (MD) -8.52 (95 % confidence interval (CI) -14.56, -2.49) min] as well as lower relative risk for postoperative complications [risk ratio (RR) 0.86 (0.75, 0.99)] and nausea and vomiting [RR 0.58 (0.51, 0.66)]. There were no significant differences in estimated blood loss [MD -27.59 (-61.85, -9.97) ml], hospital stay duration [MD -1.6 (-3.95, 0.75) d], pain [MD -0.22 (-1.35, 0.92) VAS] and disability scales [MD -0.8 (-3.54, 1.94) ODI]. Selected studies were considerably heterogeneic (<i>I</i> <sup><i>2</i></sup> = 0-99.89 %).</p><p><strong>Discussion and conclusion: </strong>Awake surgery is a safe and promising alternative to GA in decompressive spine surgery, however, high heterogeneity of the present literature warrant confirmation in future prospective, randomized trials.</p>","PeriodicalId":72443,"journal":{"name":"Brain & spine","volume":"5 ","pages":"104280"},"PeriodicalIF":2.5000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12147886/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain & spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.bas.2025.104280","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Decompressive lumbar spine surgery is a common procedure for disc herniation and spinal stenosis. Besides intervention under general anesthesia (GA), awake surgery (AS) in local or spinal anesthesia offers potential benefits regarding GA-related side effects and simplified periprocedural management.
Research question: Within this systematic analysis, we sought to compare postsurgical outcomes of spinal decompression surgeries in GA and AS.
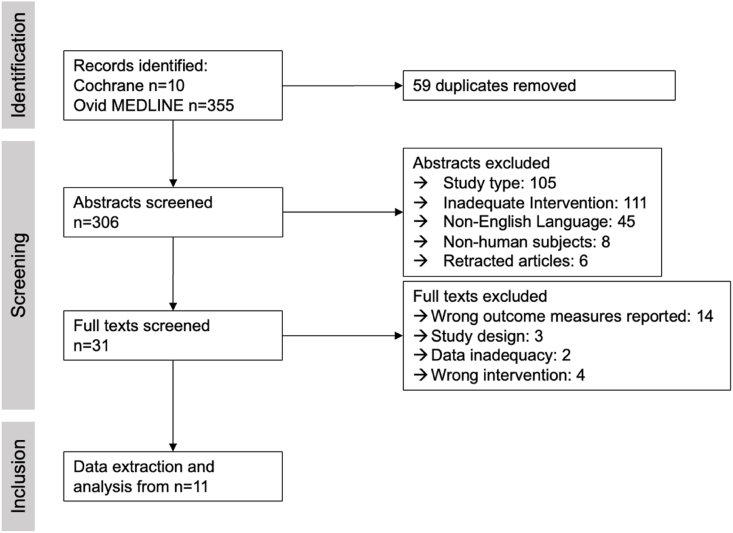
Methods: Following the PRISMA guidelines, we extracted all relevant studies from three databases and collected all data concerning surgery duration, blood loss, postoperative duration of hospitalization, postoperative pain (VAS), and disability indices (ODI).
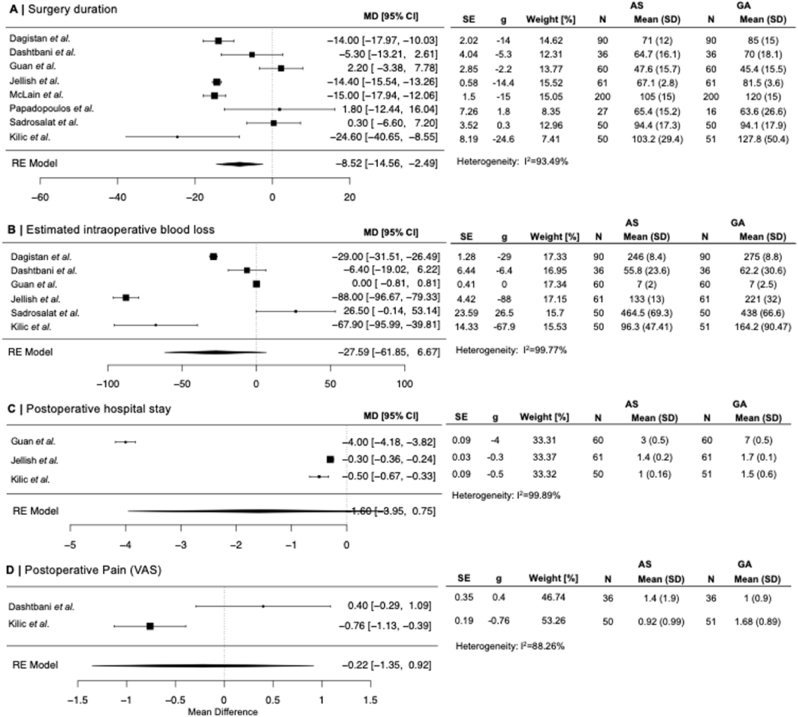
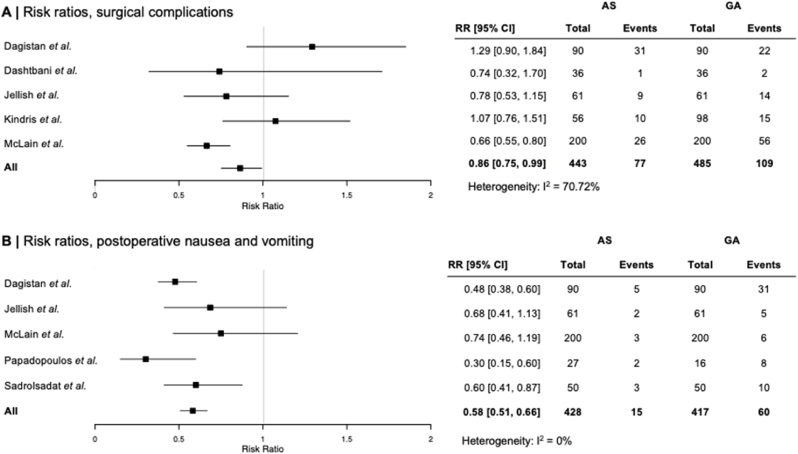
Results: In total, we identified 11 studies covering 1350 patients. AS was associated with shorter surgery duration [Mean difference (MD) -8.52 (95 % confidence interval (CI) -14.56, -2.49) min] as well as lower relative risk for postoperative complications [risk ratio (RR) 0.86 (0.75, 0.99)] and nausea and vomiting [RR 0.58 (0.51, 0.66)]. There were no significant differences in estimated blood loss [MD -27.59 (-61.85, -9.97) ml], hospital stay duration [MD -1.6 (-3.95, 0.75) d], pain [MD -0.22 (-1.35, 0.92) VAS] and disability scales [MD -0.8 (-3.54, 1.94) ODI]. Selected studies were considerably heterogeneic (I2 = 0-99.89 %).
Discussion and conclusion: Awake surgery is a safe and promising alternative to GA in decompressive spine surgery, however, high heterogeneity of the present literature warrant confirmation in future prospective, randomized trials.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


