Asma A Adan, Redemtor A Ojuang, Steven G Nyanjom, Edward K Maina
{"title":"Prevalence of thyroid dysfunction in highly active antiretroviral therapy -Exposed people living with human immunodeficiency virus.","authors":"Asma A Adan, Redemtor A Ojuang, Steven G Nyanjom, Edward K Maina","doi":"10.1186/s13044-025-00240-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The incidence of thyroid dysfunction is high in HIV patients, contributing to the high mortality and morbidity associated with HIV.</p><p><strong>Objectives: </strong>This study focused on evaluating the prevalence of thyroid dysfunction and associated factors among people living with HIV (PLWH) attending Comprehensive care centre at Maua Methodist Hospital, Kenya.</p><p><strong>Methods: </strong>Clinical and sociodemographic data of participants were collected including HIV viral loads, CD4 counts, HAART regimen and type, age, gender, marital and education status, and co-infection. Serum levels of thyroid-stimulating hormone (TSH), free thyroxine (FT4), and free triiodothyronine (FT3) were assessed in all groups. Regression analysis and Pearson correlation were performed to assess thyroid dysfunction and associated factors.</p><p><strong>Results: </strong>The prevalence of thyroid dysfunction was 51.9% (95% CI: 50.8 ~ 53.2) in this population. 77% (77%) of the HAART group had thyroid dysfunction compared to 47% of the HAART naïve group. Additionally, the prevalence of thyroid dysfunction was high in the HIV-non-suppressed individuals (97%, 95% CI: 97.1 ~ 97.9) compared to suppressed group (83%, 95% CI: 82.7 ~ 84.3). HIV (p < 0.001), HAART exposure (p < 0.001), TB (p < 0.001) and duration of infection (p = 0.002) were significantly associated with thyroid dysfunction. There was a positive correlation between TSH (r = 0.28; p < 0.01) and HIV + individuals under HAART, TSH (r = 0.37; p < 0.001) and TB, and FT3 (r = 0.35; p < 0.001) and duration of infection. Additionally, there was positive corelation between thyroid dysfunction and age (r = 0.13, p = 0.13), and a negative correlation between thyroid dysfunction and CD4 counts (r = -0.39, p < 0.055) though statistically not significant.</p><p><strong>Conclusions: </strong>Thyroid dysfunction is more common in HIV patients on HAART, mainly manifested as subclinical hypothyroidism. Routine screening for thyroid dysfunction should be considered for PLWH, especially those on HAART and with viral blips.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":"18 1","pages":"24"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12150516/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-025-00240-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The incidence of thyroid dysfunction is high in HIV patients, contributing to the high mortality and morbidity associated with HIV.
Objectives: This study focused on evaluating the prevalence of thyroid dysfunction and associated factors among people living with HIV (PLWH) attending Comprehensive care centre at Maua Methodist Hospital, Kenya.
Methods: Clinical and sociodemographic data of participants were collected including HIV viral loads, CD4 counts, HAART regimen and type, age, gender, marital and education status, and co-infection. Serum levels of thyroid-stimulating hormone (TSH), free thyroxine (FT4), and free triiodothyronine (FT3) were assessed in all groups. Regression analysis and Pearson correlation were performed to assess thyroid dysfunction and associated factors.
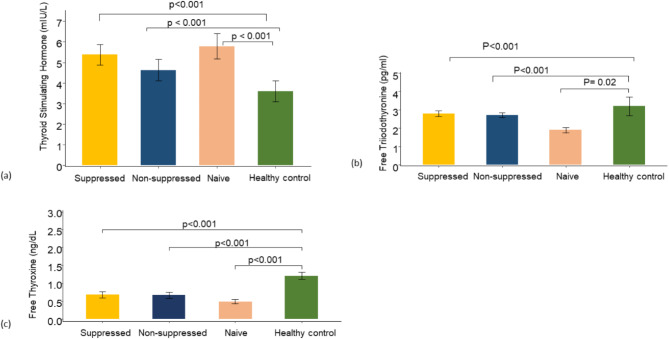
Results: The prevalence of thyroid dysfunction was 51.9% (95% CI: 50.8 ~ 53.2) in this population. 77% (77%) of the HAART group had thyroid dysfunction compared to 47% of the HAART naïve group. Additionally, the prevalence of thyroid dysfunction was high in the HIV-non-suppressed individuals (97%, 95% CI: 97.1 ~ 97.9) compared to suppressed group (83%, 95% CI: 82.7 ~ 84.3). HIV (p < 0.001), HAART exposure (p < 0.001), TB (p < 0.001) and duration of infection (p = 0.002) were significantly associated with thyroid dysfunction. There was a positive correlation between TSH (r = 0.28; p < 0.01) and HIV + individuals under HAART, TSH (r = 0.37; p < 0.001) and TB, and FT3 (r = 0.35; p < 0.001) and duration of infection. Additionally, there was positive corelation between thyroid dysfunction and age (r = 0.13, p = 0.13), and a negative correlation between thyroid dysfunction and CD4 counts (r = -0.39, p < 0.055) though statistically not significant.
Conclusions: Thyroid dysfunction is more common in HIV patients on HAART, mainly manifested as subclinical hypothyroidism. Routine screening for thyroid dysfunction should be considered for PLWH, especially those on HAART and with viral blips.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


