{"title":"Intraoperative hypotension during robotic-assisted radical prostatectomy: A randomised controlled trial comparing standard goal-directed fluid therapy with hypotension prediction index-guided goal-directed fluid therapy.","authors":"Cotoia Antonella, Antonello Discenza, Michela Rauseo, Mario Matella, Girolamo Caggianelli, Rossana Ciaramelletti, Lucia Mirabella, Gilda Cinnella","doi":"10.1097/EJA.0000000000002211","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Robot-assisted radical prostatectomy (RARP) represents the leading application of robotic surgery in the treatment for prostate cancer with faster recovery and reduced invasiveness. Maintaining stable blood pressure during RARP is crucial to avoid complications. The approach used is goal-directed therapy (GDT); however, the Hypotension Prediction Index (HPI), a machine learning algorithm that analyses arterial waveforms, may provide additional benefits.</p><p><strong>Objective: </strong>To evaluate the cumulative amount, frequency and duration of intraoperative hypotension episodes in patients undergoing RARP, comparing those managed with a GDT protocol guided by the HPI algorithm versus those managed without it.</p><p><strong>Design: </strong>Prospective randomised study.</p><p><strong>Setting: </strong>Single-centre university hospital. Recruitment from January 2022 to April 2023.</p><p><strong>Participants: </strong>Eighty-two patients.</p><p><strong>Interventions: </strong>Patients undergoing RARP were randomly assigned to either a GDT protocol alone (control) or a GDT protocol guided by the HPI (HPI group). All patients received both general anaesthesia and a single-shot spinal technique.</p><p><strong>Mean outcome measures: </strong>Cumulative amount of intraoperative hypotension [measured using the time-weighted average (TWA) of mean arterial pressure (MAP) below 65 mmHg]; frequency of hypotensive events; duration of hypotensive events; postoperative complications; length of stay.</p><p><strong>Results: </strong>No differences were observed in TWA-MAP, or in the frequency and duration of hypotensive events between the groups. Both groups maintained stable haemodynamics with minimal hypotension, and had similar fluid infusion and vasoconstrictor administration. Additionally, there were no differences in postoperative complications or length of stay.</p><p><strong>Conclusions: </strong>In our study, HPI guidance did not reduce intraoperative hypotension during RARP. Interestingly, the control group experienced fewer hypotensive events than typically reported in the literature, likely because of the high standards of haemodynamic and anaesthesiologic management maintained across both groups.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov identifier: NCT06535464.</p>","PeriodicalId":11920,"journal":{"name":"European Journal of Anaesthesiology","volume":" ","pages":"916-923"},"PeriodicalIF":6.8000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422612/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Anaesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/EJA.0000000000002211","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Robot-assisted radical prostatectomy (RARP) represents the leading application of robotic surgery in the treatment for prostate cancer with faster recovery and reduced invasiveness. Maintaining stable blood pressure during RARP is crucial to avoid complications. The approach used is goal-directed therapy (GDT); however, the Hypotension Prediction Index (HPI), a machine learning algorithm that analyses arterial waveforms, may provide additional benefits.
Objective: To evaluate the cumulative amount, frequency and duration of intraoperative hypotension episodes in patients undergoing RARP, comparing those managed with a GDT protocol guided by the HPI algorithm versus those managed without it.
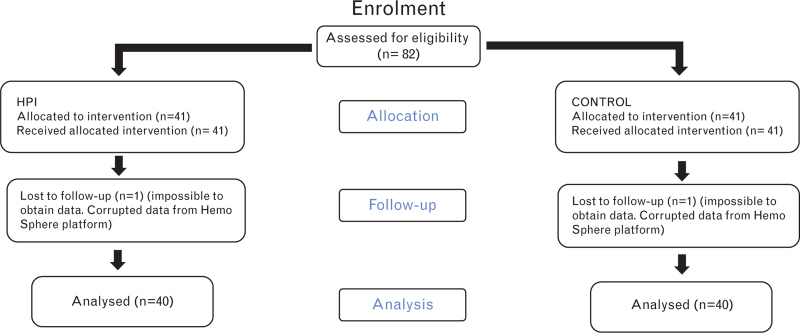
Design: Prospective randomised study.
Setting: Single-centre university hospital. Recruitment from January 2022 to April 2023.
Participants: Eighty-two patients.
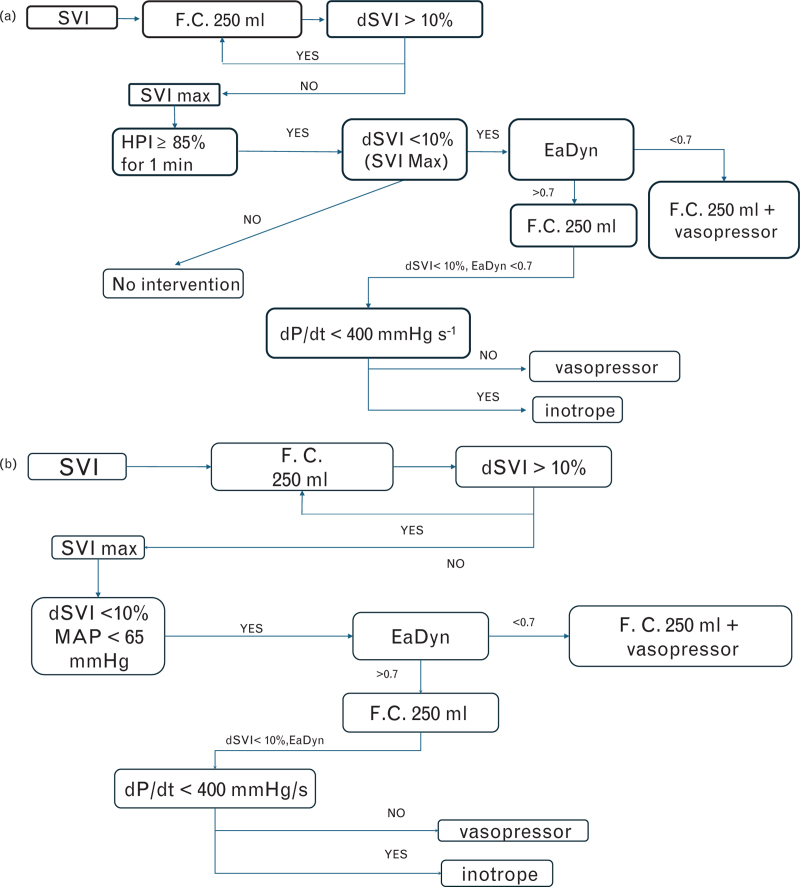
Interventions: Patients undergoing RARP were randomly assigned to either a GDT protocol alone (control) or a GDT protocol guided by the HPI (HPI group). All patients received both general anaesthesia and a single-shot spinal technique.
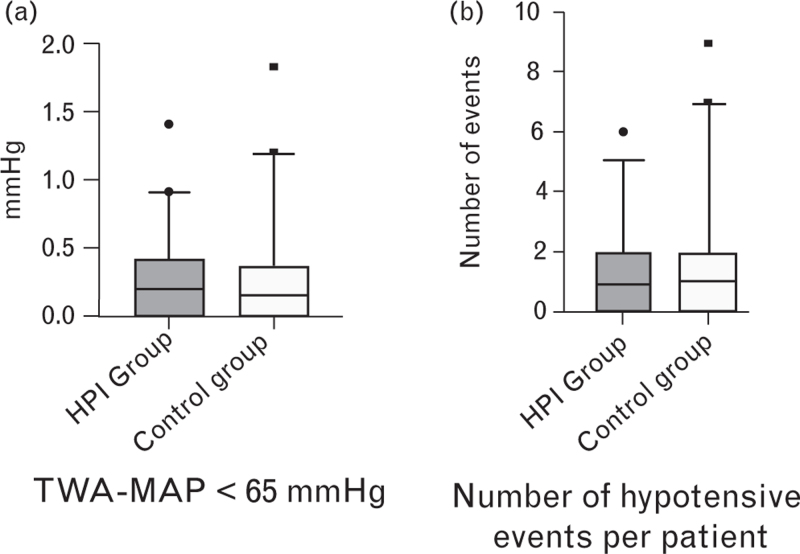
Mean outcome measures: Cumulative amount of intraoperative hypotension [measured using the time-weighted average (TWA) of mean arterial pressure (MAP) below 65 mmHg]; frequency of hypotensive events; duration of hypotensive events; postoperative complications; length of stay.
Results: No differences were observed in TWA-MAP, or in the frequency and duration of hypotensive events between the groups. Both groups maintained stable haemodynamics with minimal hypotension, and had similar fluid infusion and vasoconstrictor administration. Additionally, there were no differences in postoperative complications or length of stay.
Conclusions: In our study, HPI guidance did not reduce intraoperative hypotension during RARP. Interestingly, the control group experienced fewer hypotensive events than typically reported in the literature, likely because of the high standards of haemodynamic and anaesthesiologic management maintained across both groups.
期刊介绍:
The European Journal of Anaesthesiology (EJA) publishes original work of high scientific quality in the field of anaesthesiology, pain, emergency medicine and intensive care. Preference is given to experimental work or clinical observation in man, and to laboratory work of clinical relevance. The journal also publishes commissioned reviews by an authority, editorials, invited commentaries, special articles, pro and con debates, and short reports (correspondences, case reports, short reports of clinical studies).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


