The impact of lifestyle modification on metabolic pathways in older adults with overweight/obesity and rheumatoid arthritis: a secondary exploratory analysis of the SWET-RA study.
Grace Kim, Leanna M Ross, Alyssa M Sudnick, Johanna L Johnson, Carl F Pieper, Margery A Connelly, Olga Ilkayeva, Michael J Muehlbauer, Connie W Bales, Kathryn N Porter Starr, William E Kraus, Brian J Andonian, Kim M Huffman
{"title":"The impact of lifestyle modification on metabolic pathways in older adults with overweight/obesity and rheumatoid arthritis: a secondary exploratory analysis of the SWET-RA study.","authors":"Grace Kim, Leanna M Ross, Alyssa M Sudnick, Johanna L Johnson, Carl F Pieper, Margery A Connelly, Olga Ilkayeva, Michael J Muehlbauer, Connie W Bales, Kathryn N Porter Starr, William E Kraus, Brian J Andonian, Kim M Huffman","doi":"10.1186/s41927-025-00525-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rheumatoid arthritis (RA) is associated with increased cardiometabolic risk due to inflammation and traditional risk factors, both of which can be mitigated by lifestyle modifications. This study examines metabolic pathways influenced by lifestyle changes and related to improved cardiometabolic risk.</p><p><strong>Methods: </strong>This is a secondary exploratory analysis of the Supervised Weight loss and Exercise Training (SWET) study, in which twenty older adults with RA and overweight/obesity were randomized to 16 weeks of SWET or a counseling program. Baseline and post-intervention measures included mass spectrometry (MS) and nuclear magnetic resonance (NMR) metabolites and lipoproteins; cardiometabolic risk parameters; and RA clinical outcomes. Principal components analysis (PCA) reduced MS change scores into change factors. Between-group differences were assessed with t-tests and linear regression. Within-group differences were assessed with Wilcoxon-signed rank tests. Spearman's rank correlated MS change factors and NMR change scores with clinical outcomes.</p><p><strong>Results: </strong>Group differences were minimal. In all participants, improvements in metabolic syndrome score were associated with increases in PCA Factor 1 (short- and medium-chain acylcarnitines) and ketone bodies (ρ=-0.57, unadjusted p = 0.009, adjusted p = 0.04; ρ=-0.45, unadjusted p = 0.049, adjusted p = 1.00) and decreases in large low-density lipoprotein particles (LDLp) and large high-density lipoprotein particles (HDLp) (ρ = 0.48, unadjusted p = 0.03, adjusted p = 1.00; ρ = 0.48, unadjusted p = 0.03, adjusted p = 1.00). Improvements in RA disease activity (DAS-28<sub>ESR</sub>) were associated with reductions in very large triglyceride-rich lipoprotein particles (TRLp) (ρ = 0.60, unadjusted p = 0.01, adjusted p = 0.48). Improvements in patient-reported physical health were associated with reductions in HDL-c, ApoA1 concentrations, and medium HDLp (ρ=-0.50, unadjusted p = 0.03, adjusted p = 1.00; ρ=-0.47, unadjusted p = 0.04, adjusted p = 1.00; ρ=-0.45, unadjusted p = 0.047, adjusted p = 1.00). Improvements in patient-reported mental health were associated with decreases in high-density lipoprotein 6 (H6) particles (ρ=-0.60, unadjusted p = 0.03, adjusted p = 1.00), medium HDLp (ρ=-0.54, unadjusted p = 0.01, adjusted p = 0.48), and LDL size (ρ=-0.52, unadjusted p = 0.02, adjusted p = 0.96).</p><p><strong>Conclusion: </strong>In older adults with RA and overweight/obesity, both intensive supervised weight loss and exercise and lifestyle-based counseling influenced metabolic pathways, enhancing lipid metabolism (e.g., reductions in large LDLp) and metabolic flexibility (e.g., increases in fasting ketones and short- and medium-chain acylcarnitines). However, reductions in HDL-related measures should be interpreted cautiously as they may not reflect improved cardiometabolic risk.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov, NCT04356183, 04/17/2020.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"9 1","pages":"68"},"PeriodicalIF":2.5000,"publicationDate":"2025-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12147280/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-025-00525-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rheumatoid arthritis (RA) is associated with increased cardiometabolic risk due to inflammation and traditional risk factors, both of which can be mitigated by lifestyle modifications. This study examines metabolic pathways influenced by lifestyle changes and related to improved cardiometabolic risk.
Methods: This is a secondary exploratory analysis of the Supervised Weight loss and Exercise Training (SWET) study, in which twenty older adults with RA and overweight/obesity were randomized to 16 weeks of SWET or a counseling program. Baseline and post-intervention measures included mass spectrometry (MS) and nuclear magnetic resonance (NMR) metabolites and lipoproteins; cardiometabolic risk parameters; and RA clinical outcomes. Principal components analysis (PCA) reduced MS change scores into change factors. Between-group differences were assessed with t-tests and linear regression. Within-group differences were assessed with Wilcoxon-signed rank tests. Spearman's rank correlated MS change factors and NMR change scores with clinical outcomes.
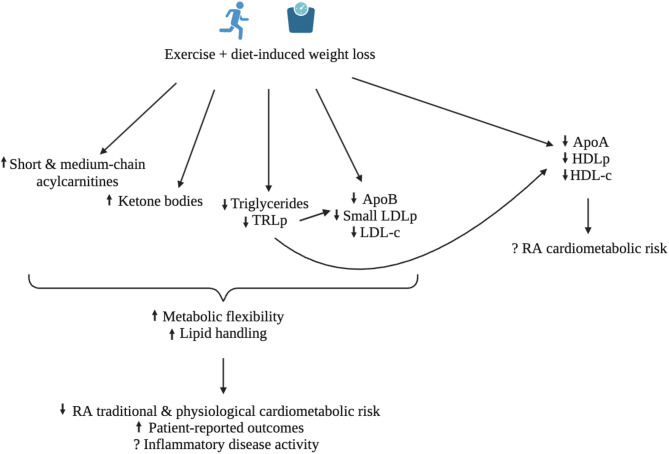
Results: Group differences were minimal. In all participants, improvements in metabolic syndrome score were associated with increases in PCA Factor 1 (short- and medium-chain acylcarnitines) and ketone bodies (ρ=-0.57, unadjusted p = 0.009, adjusted p = 0.04; ρ=-0.45, unadjusted p = 0.049, adjusted p = 1.00) and decreases in large low-density lipoprotein particles (LDLp) and large high-density lipoprotein particles (HDLp) (ρ = 0.48, unadjusted p = 0.03, adjusted p = 1.00; ρ = 0.48, unadjusted p = 0.03, adjusted p = 1.00). Improvements in RA disease activity (DAS-28ESR) were associated with reductions in very large triglyceride-rich lipoprotein particles (TRLp) (ρ = 0.60, unadjusted p = 0.01, adjusted p = 0.48). Improvements in patient-reported physical health were associated with reductions in HDL-c, ApoA1 concentrations, and medium HDLp (ρ=-0.50, unadjusted p = 0.03, adjusted p = 1.00; ρ=-0.47, unadjusted p = 0.04, adjusted p = 1.00; ρ=-0.45, unadjusted p = 0.047, adjusted p = 1.00). Improvements in patient-reported mental health were associated with decreases in high-density lipoprotein 6 (H6) particles (ρ=-0.60, unadjusted p = 0.03, adjusted p = 1.00), medium HDLp (ρ=-0.54, unadjusted p = 0.01, adjusted p = 0.48), and LDL size (ρ=-0.52, unadjusted p = 0.02, adjusted p = 0.96).
Conclusion: In older adults with RA and overweight/obesity, both intensive supervised weight loss and exercise and lifestyle-based counseling influenced metabolic pathways, enhancing lipid metabolism (e.g., reductions in large LDLp) and metabolic flexibility (e.g., increases in fasting ketones and short- and medium-chain acylcarnitines). However, reductions in HDL-related measures should be interpreted cautiously as they may not reflect improved cardiometabolic risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


