{"title":"Use of seated positioning device (Smoltap<sup>®</sup>) for ultrasound-guided infant lumbar punctures.","authors":"Shimwoo Lee, Joseph Miller","doi":"10.1007/s00247-025-06291-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Infant lumbar punctures (LPs) frequently fail at bedside and prompt repeat attempts with image guidance. Conventionally, image-guided LPs are performed with ultrasound or fluoroscopy while infants are in lateral flexed position. The procedure requires infants to be either sedated or held manually to maintain stable positioning. A new commercially available positioning device (Smoltap<sup>®</sup>) provides an alternative method to secure infants in sitting position without needing to administer sedation.</p><p><strong>Objective: </strong>To evaluate the effectiveness and safety of an infant positioning device during image-guided LPs as an alternative to the conventional LP technique.</p><p><strong>Materials and methods: </strong>We conducted a retrospective analysis of image-guided LPs from May 2022 to April 2025, approximately 1.5 years before and after the introduction of an infant positioning device in October 2023 at our institution. The device was used for awake infants stable on room air and with head-to-toe length < 57 cm, per instructions for use. The infants were secured in the device, and LPs were performed with ultrasound guidance. Patient demographics and procedural outcomes of LPs performed with and without the device were compared.</p><p><strong>Results: </strong>We analyzed 42 LPs performed with the device (\"device\" group) and 37 LPs performed without (\"no device\" group). The two groups had similar patient characteristics and rates of prior failed bedside LPs (95% and 86%, respectively, P = 0.17). The success rates of obtaining adequate CSF for microbial culture were comparable between the groups (93% and 84%, P = 0.21). There were no complications in either group. The average procedure duration was also similar (14 min vs 16 min, P = 0.65). There was no statistically significant difference in the proportions of traumatic taps when defined as CSF containing ≥ 10,000 erythrocytes/µL (26% and 16%, P = 0.42). When defined as ≥ 500 erythrocytes/µL, the rates of traumatic taps were significantly different (72% and 42%, P = 0.01). Subgroup analysis of the \"no device\" group suggested that this difference could be attributed to inclusion of sedated patients in the \"no device\" group. In the \"device\" group, no patients received sedation.</p><p><strong>Conclusion: </strong>Performing image-guided infant LPs with a positioning device is a feasible and safe alternative to the conventional technique with the benefit of not needing to sedate or manually hold infants.</p>","PeriodicalId":19755,"journal":{"name":"Pediatric Radiology","volume":" ","pages":"1591-1597"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12321679/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00247-025-06291-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/9 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
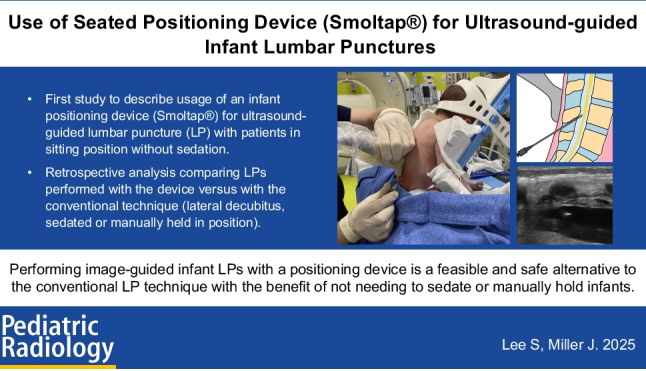
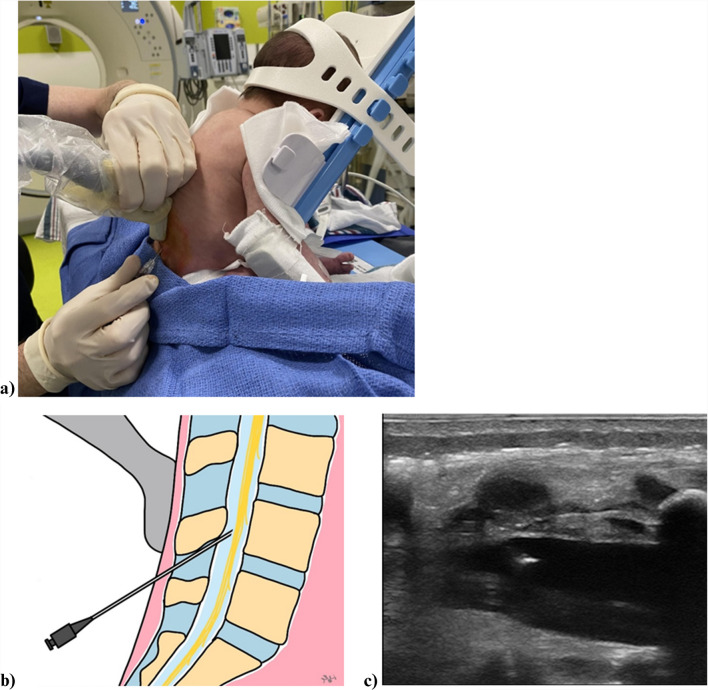
Background: Infant lumbar punctures (LPs) frequently fail at bedside and prompt repeat attempts with image guidance. Conventionally, image-guided LPs are performed with ultrasound or fluoroscopy while infants are in lateral flexed position. The procedure requires infants to be either sedated or held manually to maintain stable positioning. A new commercially available positioning device (Smoltap®) provides an alternative method to secure infants in sitting position without needing to administer sedation.
Objective: To evaluate the effectiveness and safety of an infant positioning device during image-guided LPs as an alternative to the conventional LP technique.
Materials and methods: We conducted a retrospective analysis of image-guided LPs from May 2022 to April 2025, approximately 1.5 years before and after the introduction of an infant positioning device in October 2023 at our institution. The device was used for awake infants stable on room air and with head-to-toe length < 57 cm, per instructions for use. The infants were secured in the device, and LPs were performed with ultrasound guidance. Patient demographics and procedural outcomes of LPs performed with and without the device were compared.
Results: We analyzed 42 LPs performed with the device ("device" group) and 37 LPs performed without ("no device" group). The two groups had similar patient characteristics and rates of prior failed bedside LPs (95% and 86%, respectively, P = 0.17). The success rates of obtaining adequate CSF for microbial culture were comparable between the groups (93% and 84%, P = 0.21). There were no complications in either group. The average procedure duration was also similar (14 min vs 16 min, P = 0.65). There was no statistically significant difference in the proportions of traumatic taps when defined as CSF containing ≥ 10,000 erythrocytes/µL (26% and 16%, P = 0.42). When defined as ≥ 500 erythrocytes/µL, the rates of traumatic taps were significantly different (72% and 42%, P = 0.01). Subgroup analysis of the "no device" group suggested that this difference could be attributed to inclusion of sedated patients in the "no device" group. In the "device" group, no patients received sedation.
Conclusion: Performing image-guided infant LPs with a positioning device is a feasible and safe alternative to the conventional technique with the benefit of not needing to sedate or manually hold infants.
期刊介绍:
Official Journal of the European Society of Pediatric Radiology, the Society for Pediatric Radiology and the Asian and Oceanic Society for Pediatric Radiology
Pediatric Radiology informs its readers of new findings and progress in all areas of pediatric imaging and in related fields. This is achieved by a blend of original papers, complemented by reviews that set out the present state of knowledge in a particular area of the specialty or summarize specific topics in which discussion has led to clear conclusions. Advances in technology, methodology, apparatus and auxiliary equipment are presented, and modifications of standard techniques are described.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1964 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


