Kacper Koczyk, Arkadiusz Nowak, Marcin M Machnicki, Łukasz Zdzisław Michałowski, Edyta Maj, Tomasz Stoklosa, Przemysław Kunert
{"title":"Intramedullary Glioblastoma as One of Multiple Radiation-Induced Neoplasms.","authors":"Kacper Koczyk, Arkadiusz Nowak, Marcin M Machnicki, Łukasz Zdzisław Michałowski, Edyta Maj, Tomasz Stoklosa, Przemysław Kunert","doi":"10.1159/000545250","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Intramedullary glioblastoma is a rare entity comprising 1.4-9% of spinal gliomas. Spinal cord radiation-induced gliomas are unique, with only 13 cases reported to date.</p><p><strong>Case presentation: </strong>A 53-year-old female with a history of mediastinal Hodgkin lymphoma treated with chemotherapy and radiotherapy who subsequently developed thyroid cancer and breast cancer throughout her life was admitted due to slowly progressing spastic tetraparesis. Cervical MRI revealed an intramedullary lesion at the C4-T1 level, enlarging the spinal cord, with a heterogenous contrast enhancement and a lesion within T1 vertebral body showing contrast enhancement. Whole-body <sup>18</sup>F-FDG-PET/CT revealed increased radionuclide uptake within the cervical spinal cord at the C2-C7 level and a focus of increased metabolic activity within the T1 vertebral body. The patient underwent a C4-T2 laminectomy with tumor debulking, and a biopsy of the T1 vertebral body was taken. Closure was performed with thecal sac expansion using a fascia lata graft and open-door laminoplasty. The histomolecular results confirmed the diagnosis of glioblastoma, IDH-wildtype (CNS WHO G4), in the cervical spinal cord lesion and breast cancer metastasis in the T1 vertebral body. Postoperatively, the patient experienced progression of lower extremities and left arm paresis. No adjuvant therapy was administered due to neurological deficit progression. The patient died 6 months after surgery.</p><p><strong>Conclusion: </strong>We report a case of an intramedullary glioblastoma in a patient with a history of radiation and multiple neoplasms located at the irradiation field borders. The full molecular analysis allowed for classification of the tumor as glioblastoma, IDH-wildtype (CNS WHO G4), and screening for germinal mutations potentially predisposing to spontaneous neoplasm development.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"682-693"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143871/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545250","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Intramedullary glioblastoma is a rare entity comprising 1.4-9% of spinal gliomas. Spinal cord radiation-induced gliomas are unique, with only 13 cases reported to date.
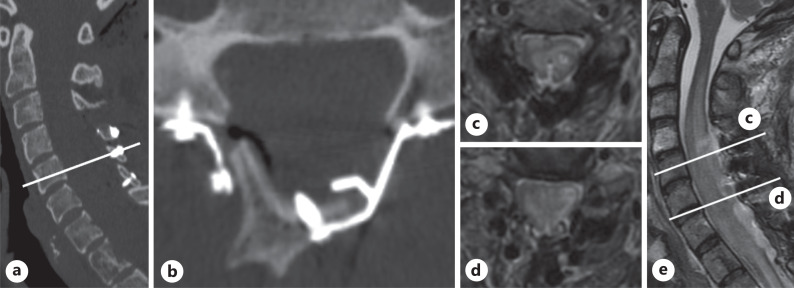
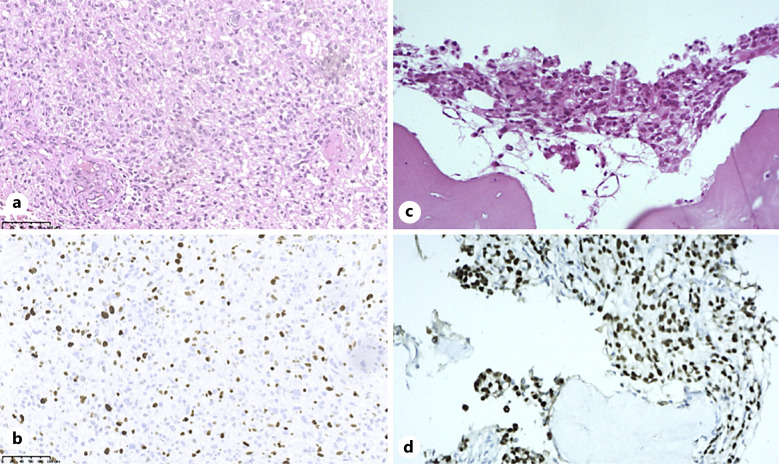
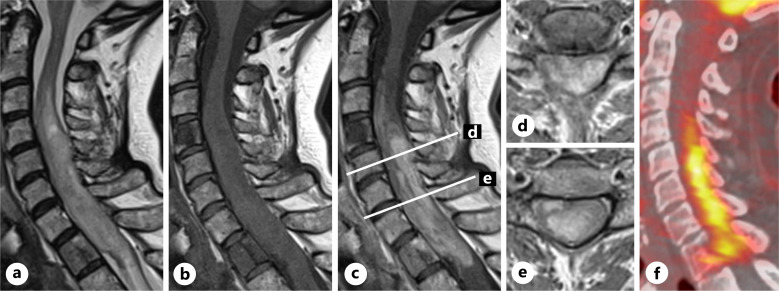
Case presentation: A 53-year-old female with a history of mediastinal Hodgkin lymphoma treated with chemotherapy and radiotherapy who subsequently developed thyroid cancer and breast cancer throughout her life was admitted due to slowly progressing spastic tetraparesis. Cervical MRI revealed an intramedullary lesion at the C4-T1 level, enlarging the spinal cord, with a heterogenous contrast enhancement and a lesion within T1 vertebral body showing contrast enhancement. Whole-body 18F-FDG-PET/CT revealed increased radionuclide uptake within the cervical spinal cord at the C2-C7 level and a focus of increased metabolic activity within the T1 vertebral body. The patient underwent a C4-T2 laminectomy with tumor debulking, and a biopsy of the T1 vertebral body was taken. Closure was performed with thecal sac expansion using a fascia lata graft and open-door laminoplasty. The histomolecular results confirmed the diagnosis of glioblastoma, IDH-wildtype (CNS WHO G4), in the cervical spinal cord lesion and breast cancer metastasis in the T1 vertebral body. Postoperatively, the patient experienced progression of lower extremities and left arm paresis. No adjuvant therapy was administered due to neurological deficit progression. The patient died 6 months after surgery.
Conclusion: We report a case of an intramedullary glioblastoma in a patient with a history of radiation and multiple neoplasms located at the irradiation field borders. The full molecular analysis allowed for classification of the tumor as glioblastoma, IDH-wildtype (CNS WHO G4), and screening for germinal mutations potentially predisposing to spontaneous neoplasm development.
髓内胶质母细胞瘤是一种罕见的实体,占脊髓胶质瘤的1.4-9%。脊髓放射诱导的神经胶质瘤是一种独特的疾病,迄今为止仅报道了13例。病例介绍:一名53岁女性,有纵隔霍奇金淋巴瘤病史,曾接受化疗和放疗,后来终生发展为甲状腺癌和乳腺癌,因缓慢进展的痉挛性四肢麻痹入院。颈椎MRI显示C4-T1水平髓内病变,脊髓增大,呈异质增强,T1椎体内病变呈增强。全身18F-FDG-PET/CT显示C2-C7水平颈脊髓内放射性核素摄取增加,T1椎体内代谢活动增加。患者行C4-T2椎板切除术,切除肿瘤,并对T1椎体进行活检。使用阔筋膜移植术和开门椎板成形术进行鞘囊扩张。组织分子检查结果证实颈脊髓病变为胶质母细胞瘤,idh -野生型(CNS WHO G4), T1椎体乳腺癌转移。术后,患者出现下肢进展和左臂麻痹。由于神经功能障碍进展,未给予辅助治疗。患者术后6个月死亡。结论:我们报告一例髓内胶质母细胞瘤,患者有放射史,多发肿瘤位于放射场边界。完整的分子分析允许将肿瘤分类为胶质母细胞瘤,idh野生型(CNS WHO G4),并筛选可能导致自发肿瘤发展的生发突变。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


