{"title":"Updated Protocol for Stroke Code Management in Prehospital Settings: The Iranian Comprehensive Stroke Code Management Program (ICSCM Phase II).","authors":"Shayan Alijanpour, Fatemeh Bahramnezhad, Ashkan Mowla, Mahdi Shafiee Sabet, Nahid Dehghan Nayeri","doi":"10.22037/aaemj.v13i1.2633","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Code stroke is a framework to reduce time and improve the quality of care in the prehospital setting. However, increased scene time, delays, and other barriers in the prehospital setting necessitate updating the current protocol. This study aimed to update the Iranian national code stroke protocol for the prehospital setting.</p><p><strong>Methods: </strong>This study represents the results of the second phase of the Iranian Comprehensive Stroke Code Management Program, a mixed methods study. We used the Caspian scientific 10-step method to update this protocol, which included a literature review, critical appraisal, extraction of recommendations, face-content validity, the Delphi method, RAND method, expert panel, stakeholders, and publishing and printing. We divided the updated protocol into three stages (on scene, ambulance care, and on admission).</p><p><strong>Results: </strong>Twenty experts (55% nurses; mean age 40.7±9.1 years, experience 15.9±7.9 years) were enrolled. On-Scene focuses on rapid ABC (airway, breathing, circulation) assessment, BEFAST (balance, eyes, face, arm, speech, and time) criteria, blood glucose check, and on-scene time under 5 minutes. Ambulance Care Involving SAMPLER (Symptoms, Allergies, Medications, Past medical history, Last time the patient was seen normally, Events leading up to the emergency medical service call, and Risk factor) history-taking, maintaining oxygen saturation ≥94%, symptom/witness documentation, electrocardiography (ECG) for cardiac-stroke cases, master's degree (MSN)-led transport coordination, and neurology team alerts and in-hospital admission ensuring precise handover, 724 pager alerts, stroke code clocks, computed tomography (CT)-ready team, and protocol updates via joint committees.</p><p><strong>Conclusion: </strong>The main points were the stroke clock, pager 724, direct delivery to computed tomography scan, administering BEFAST, and reducing scene time. We recommend that each center to enhance the infrastructure and resources for implementation of these updates. In the next phase, we will implement and evaluate this protocol.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"13 1","pages":"e43"},"PeriodicalIF":2.0000,"publicationDate":"2025-04-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12145130/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaemj.v13i1.2633","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Code stroke is a framework to reduce time and improve the quality of care in the prehospital setting. However, increased scene time, delays, and other barriers in the prehospital setting necessitate updating the current protocol. This study aimed to update the Iranian national code stroke protocol for the prehospital setting.
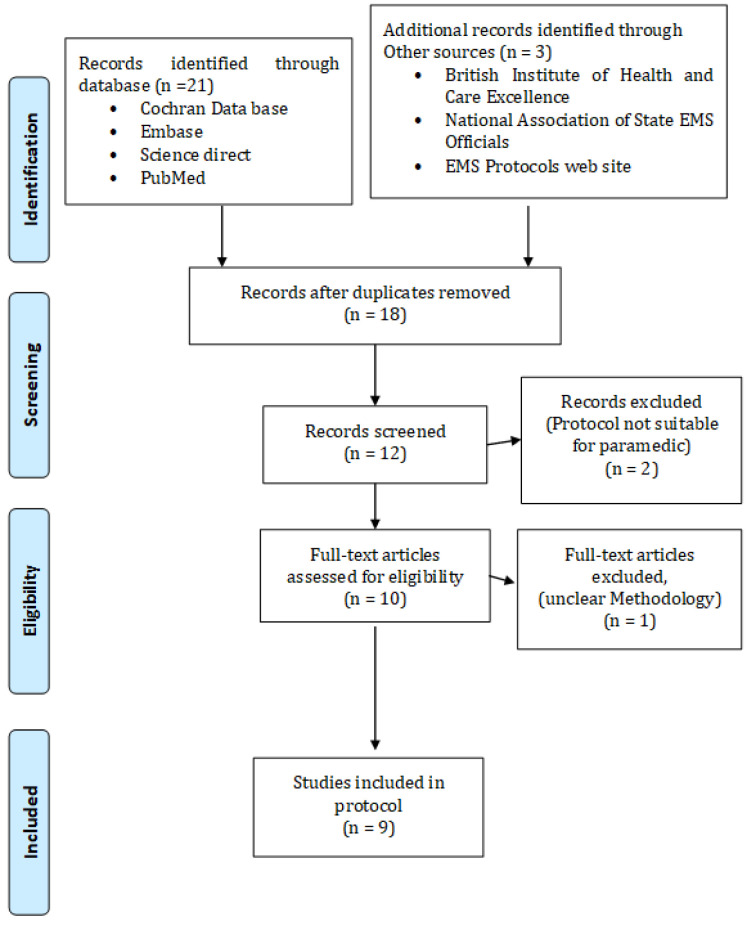
Methods: This study represents the results of the second phase of the Iranian Comprehensive Stroke Code Management Program, a mixed methods study. We used the Caspian scientific 10-step method to update this protocol, which included a literature review, critical appraisal, extraction of recommendations, face-content validity, the Delphi method, RAND method, expert panel, stakeholders, and publishing and printing. We divided the updated protocol into three stages (on scene, ambulance care, and on admission).
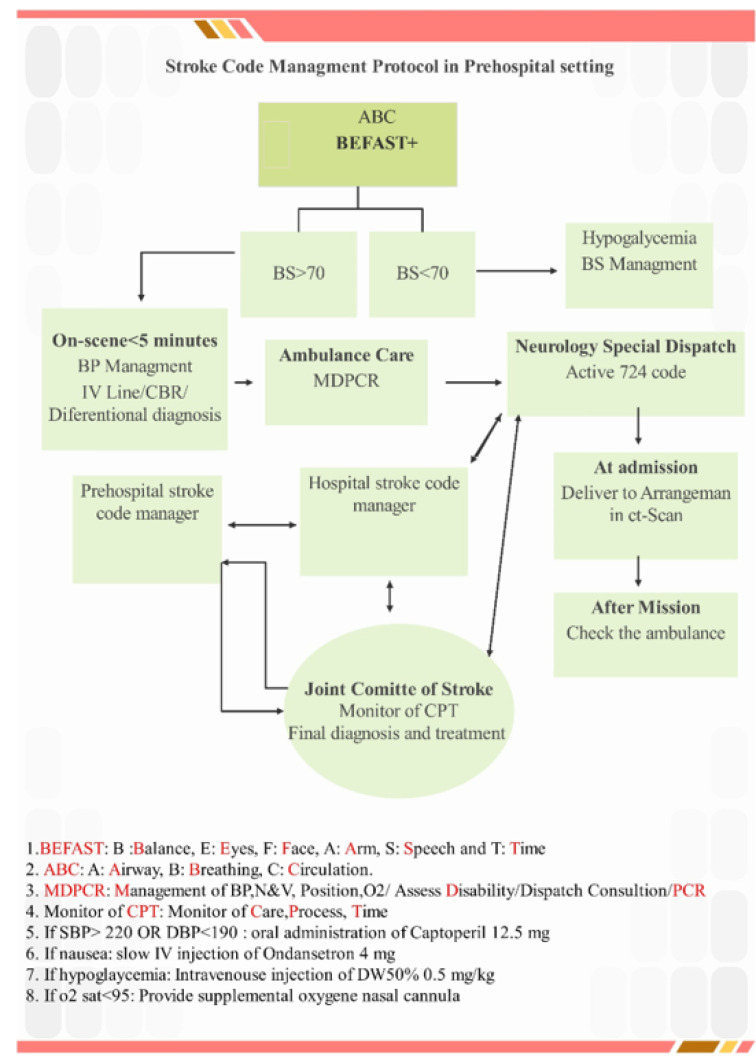
Results: Twenty experts (55% nurses; mean age 40.7±9.1 years, experience 15.9±7.9 years) were enrolled. On-Scene focuses on rapid ABC (airway, breathing, circulation) assessment, BEFAST (balance, eyes, face, arm, speech, and time) criteria, blood glucose check, and on-scene time under 5 minutes. Ambulance Care Involving SAMPLER (Symptoms, Allergies, Medications, Past medical history, Last time the patient was seen normally, Events leading up to the emergency medical service call, and Risk factor) history-taking, maintaining oxygen saturation ≥94%, symptom/witness documentation, electrocardiography (ECG) for cardiac-stroke cases, master's degree (MSN)-led transport coordination, and neurology team alerts and in-hospital admission ensuring precise handover, 724 pager alerts, stroke code clocks, computed tomography (CT)-ready team, and protocol updates via joint committees.
Conclusion: The main points were the stroke clock, pager 724, direct delivery to computed tomography scan, administering BEFAST, and reducing scene time. We recommend that each center to enhance the infrastructure and resources for implementation of these updates. In the next phase, we will implement and evaluate this protocol.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


