Valve-in-valve transcatheter aortic valve replacement versus redo surgical aortic valve replacement in patients with degenerated aortic bioprostheses: Three-year death rates and haemodynamic performance
IF 2.2
3区 医学
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
Management of degenerated aortic bioprostheses through valve-in-valve transcatheter aortic valve replacement (ViV-TAVR) or redo surgical aortic valve replacement (Re-SAVR) shows similar short-term safety and efficacy. However, long-term survival and haemodynamic performance data are limited.
Aim
To compare clinical characteristics, haemodynamics and outcomes at 3 years between ViV-TAVR and Re-SAVR techniques.
Methods
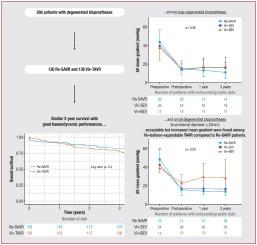
This retrospective two-centre study included 266 patients treated for isolated aortic bioprosthesis degeneration (130 Re-SAVR, 136ViV-TAVR) from 2009 to 2018, with up to 3 years of follow-up.
Results
The ViV-TAVR group was older (83 vs. 77 years; P = 0.005) with higher surgical risk (Logistic EuroSCORE 22% vs. 13%; P = 0.005). At 3 years, univariate analysis showed no significant difference in all-cause deaths (22.1% vs. 17.7%; P = 0.37). ViV-TAVR was associated with fewer first-month complications, including major bleeding (11.0% vs. 52.3%; P = 0.007) and acute renal failure grade 2/3 (5.1% vs. 14.6%; P = 0.053). Inverse probability of treatment weighting analysis revealed no difference in all-cause deaths at 1 year (hazard ratio [HR] 0.78, 95% confidence interval [CI] 0.36–1.67; P = 0.52) or between 1 and 3 years (HR 1.56, 95% CI 0.82–2.99; P = 0.17). Composite events were similar at 1 year (HR 0.80, 95% CI 0.44–1.44; P = 0.45) and between 1 and 3 years (HR 1.41, 95% CI 0.83–2.38; P = 0.21). Mean gradients at 3 years were similar (16.1 ± 11.4 vs. 13.2 ± 5.3 mmHg; P = 0.17). In patients with small bioprostheses (true internal diameter ≤ 20 mm [n = 151]), death rates at 3 years were similar (21.1% vs. 20.0%; P = 0.86), as was haemodynamic performance (mean gradient 19.2 ± 14.0 mmHg for ViV-TAVR vs. 13.7 ± 4.12 mmHg for Re-SAVR [P = 0.38]). Compared to balloon-expandable, self-expandable valves showed better 1-year mean gradients (16.4 ± 10.5 vs. 13.7 ± 4.12 mmHg; P = 0.012).
Conclusions
ViV-TAVR and Re-SAVR had similar mortality and haemodynamic outcomes at 3 years, including in patients with small bioprostheses where self-expandable valves yielded the best results.
经导管瓣内主动脉瓣置换术与重做外科主动脉瓣置换术治疗退行性主动脉瓣生物假体患者:三年死亡率和血流动力学性能。
背景:通过瓣中瓣经导管主动脉瓣置换术(ViV-TAVR)或重做手术主动脉瓣置换术(Re-SAVR)治疗退行性主动脉瓣生物假体的短期安全性和有效性相似。然而,长期生存和血流动力学性能数据有限。目的:比较ViV-TAVR和Re-SAVR技术的临床特征、血流动力学和3年预后。方法:本回顾性双中心研究纳入了2009年至2018年266例孤立性主动脉生物假体变性患者(130例Re-SAVR, 136ViV-TAVR),随访时间长达3年。结果:ViV-TAVR组患者年龄较大(83岁vs 77岁;P=0.005),手术风险较高(Logistic EuroSCORE 22%对13%;P = 0.005)。3年时,单因素分析显示全因死亡率无显著差异(22.1% vs. 17.7%;P = 0.37)。ViV-TAVR与较少的第一个月并发症相关,包括大出血(11.0% vs. 52.3%;P=0.007)和2/3级急性肾衰竭(5.1% vs. 14.6%;P = 0.053)。治疗加权逆概率分析显示,1年内全因死亡无差异(风险比[HR] 0.78, 95%可信区间[CI] 0.36-1.67;P=0.52)或1 - 3年(HR 1.56, 95% CI 0.82-2.99;P = 0.17)。1年后的综合事件相似(HR 0.80, 95% CI 0.44-1.44;P=0.45)和1 - 3年(HR 1.41, 95% CI 0.83-2.38;P = 0.21)。3年的平均梯度相似(16.1±11.4 vs 13.2±5.3mmHg;P = 0.17)。在小生物假体(真内径≤20mm [n=151])患者中,3年死亡率相似(21.1% vs. 20.0%;P=0.86),血流动力学性能也是如此(ViV-TAVR的平均梯度为19.2±14.0mmHg, Re-SAVR的平均梯度为13.7±4.12mmHg [P=0.38])。与球囊膨胀阀相比,自膨胀阀表现出更好的1年平均梯度(16.4±10.5 vs 13.7±4.12mmHg;P = 0.012)。结论:ViV-TAVR和Re-SAVR在3年时具有相似的死亡率和血流动力学结果,包括在使用小型生物假体的患者中,自膨胀瓣膜的效果最好。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Archives of Cardiovascular Diseases
医学-心血管系统
CiteScore
4.40
自引率
6.70%
发文量
87
审稿时长
34 days
期刊介绍:
The Journal publishes original peer-reviewed clinical and research articles, epidemiological studies, new methodological clinical approaches, review articles and editorials. Topics covered include coronary artery and valve diseases, interventional and pediatric cardiology, cardiovascular surgery, cardiomyopathy and heart failure, arrhythmias and stimulation, cardiovascular imaging, vascular medicine and hypertension, epidemiology and risk factors, and large multicenter studies. Archives of Cardiovascular Diseases also publishes abstracts of papers presented at the annual sessions of the Journées Européennes de la Société Française de Cardiologie and the guidelines edited by the French Society of Cardiology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


