{"title":"\"Attenuated\" Pulmonary Tumor Thrombotic Microangiopathy on Anti-Vascular Endothelial Growth Factor Treatment: A Case Report.","authors":"Haruka Ozaki, Takeshi Yamaguchi, Rika Kizawa, Yuko Tanabe, Koichi Suyama, Yuji Miura","doi":"10.1159/000543930","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Antemortem diagnosis of pulmonary tumor thrombotic microangiopathy (PTTM) is challenging because of rapidly worsening respiratory failure. Vascular endothelial growth factor (VEGF) is involved in PTTM pathogenesis; however, the clinical picture of PTTM in patients with cancer receiving anti-VEGF treatment is unknown.</p><p><strong>Case presentation: </strong>A 40-year-old man with advanced gastric adenocarcinoma on paclitaxel plus ramucirumab developed a dry cough and, after 2 months of a stable period, dyspnea on exertion. Chest computed tomography (CT) showed bilateral diffuse patchy ground-glass opacities (GGOs). Transbronchial biopsy revealed alveolar hemorrhage and small pulmonary arteries occluded with fibrocellular intimal proliferation, but no tumor cells. Suspecting chemotherapy-induced lung injury, we discontinued the chemotherapy and monitored him carefully without treatment. However, his dyspnea worsened, and follow-up chest CT showed worsening GGOs and right atrial and pulmonary arterial dilatation. Ultrasound cardiography indicated reduced right ventricular function. Lung perfusion scintigraphy confirmed numerous bilateral defects. Right heart catheterization revealed pulmonary hypertension, but no tumor cells on pulmonary wedge aspiration cytology. We clinically diagnosed the patient with PTTM. Three weeks after his initial visit for dyspnea, he was started on nivolumab. One week after treatment, he required home oxygen therapy at 1 L/min on exertion. After two doses of nivolumab, he no longer had dyspnea and discontinued oxygen therapy. Follow-up ultrasound cardiography showed normal pulmonary arterial pressure, and almost all GGOs on chest CT were resolved.</p><p><strong>Conclusion: </strong>VEGF inhibitors may attenuate PTTM symptoms. Even with mild respiratory symptoms, oncologists should consider PTTM in patients with cancer on VEGF inhibitors.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"659-666"},"PeriodicalIF":0.7000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12140605/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543930","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Antemortem diagnosis of pulmonary tumor thrombotic microangiopathy (PTTM) is challenging because of rapidly worsening respiratory failure. Vascular endothelial growth factor (VEGF) is involved in PTTM pathogenesis; however, the clinical picture of PTTM in patients with cancer receiving anti-VEGF treatment is unknown.
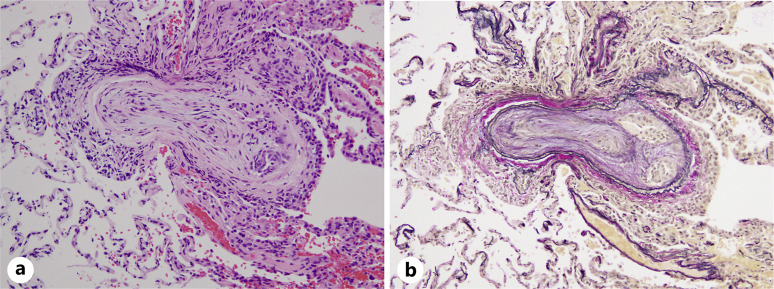
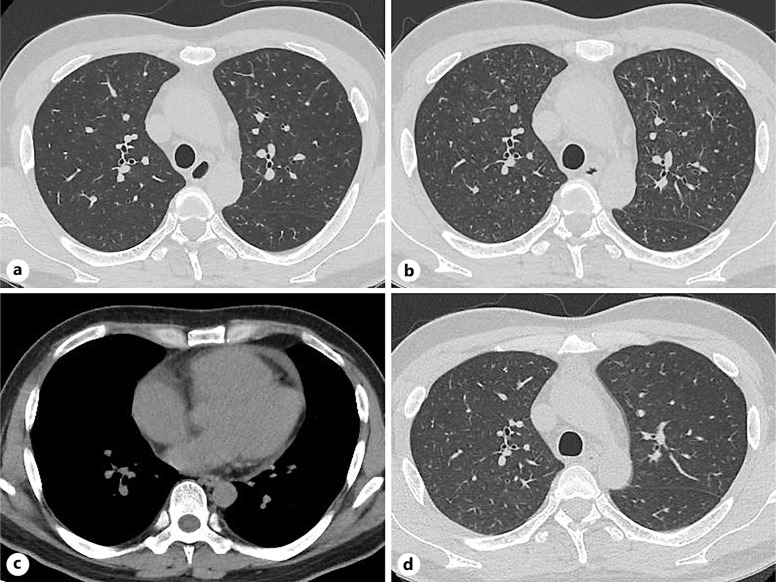
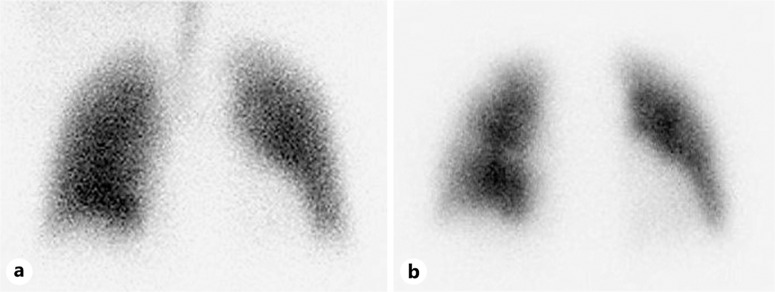
Case presentation: A 40-year-old man with advanced gastric adenocarcinoma on paclitaxel plus ramucirumab developed a dry cough and, after 2 months of a stable period, dyspnea on exertion. Chest computed tomography (CT) showed bilateral diffuse patchy ground-glass opacities (GGOs). Transbronchial biopsy revealed alveolar hemorrhage and small pulmonary arteries occluded with fibrocellular intimal proliferation, but no tumor cells. Suspecting chemotherapy-induced lung injury, we discontinued the chemotherapy and monitored him carefully without treatment. However, his dyspnea worsened, and follow-up chest CT showed worsening GGOs and right atrial and pulmonary arterial dilatation. Ultrasound cardiography indicated reduced right ventricular function. Lung perfusion scintigraphy confirmed numerous bilateral defects. Right heart catheterization revealed pulmonary hypertension, but no tumor cells on pulmonary wedge aspiration cytology. We clinically diagnosed the patient with PTTM. Three weeks after his initial visit for dyspnea, he was started on nivolumab. One week after treatment, he required home oxygen therapy at 1 L/min on exertion. After two doses of nivolumab, he no longer had dyspnea and discontinued oxygen therapy. Follow-up ultrasound cardiography showed normal pulmonary arterial pressure, and almost all GGOs on chest CT were resolved.
Conclusion: VEGF inhibitors may attenuate PTTM symptoms. Even with mild respiratory symptoms, oncologists should consider PTTM in patients with cancer on VEGF inhibitors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


