{"title":"Vancomycin Monitoring for Treatment of Acute Pulmonary Exacerbations of Adult Cystic Fibrosis Patients.","authors":"Darrell Smith, James Sanders, Marguerite Monogue","doi":"10.1155/pm/5683225","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Therapeutic drug monitoring (TDM) for vancomycin (VAN) in adult people with cystic fibrosis (pwCF) historically has utilized trough concentrations. Recent VAN TDM guidelines recommend area under the curve (AUC) monitoring to reduce the risk of acute kidney injury (AKI), despite limited evidence to support this practice in adult pwCF. <b>Methods:</b> This single-center, retrospective, observational cohort study included 143 adult pwCF admitted from July 1, 2017, to July 1, 2022, with an acute pulmonary exacerbation that received VAN for at least 72 h with available VAN plasma concentrations for TDM for AUC (<i>n</i> = 39) or trough monitoring (<i>n</i> = 104). Eligible patients with multiple hospital admissions during the study period were incorporated as separate encounters. The primary outcome was the incidence of AKI. <b>Results:</b> Receipt of concurrent nephrotoxins was more common in the AUC cohort than in the trough cohort (97% vs. 81%, <i>p</i> = 0.01), but the rate of AKI was similar (7.7% vs. 10.6%, <i>p</i> = 0.76). AUC monitoring was associated with earlier achievement of TDM goal (median 0 days (IQR 0-2) vs. 2 days (IQR 0-4), <i>p</i> < 0.01), lower total daily doses (34.8 mg/kg/day (IQR 27.6-49) vs. 57.5 mg/kg/day (IQR 43.9-68.6), <i>p</i> < 0.01), and fewer regimen changes (median 1 change (IQR 0-2) vs. 2 changes (IQR 1-3), <i>p</i> < 0.01). In patients with MRSA, pulmonary function recovery, readmission, and mortality were similar. <b>Conclusion:</b> In adult pwCF, the incidence of AKI was similar between AUC and trough monitoring cohorts; however, AUC monitoring achieved therapeutic targets sooner with fewer regimen modifications without significantly increasing the number of concentrations compared to trough monitoring.</p>","PeriodicalId":46434,"journal":{"name":"Pulmonary Medicine","volume":"2025 ","pages":"5683225"},"PeriodicalIF":2.1000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136855/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/pm/5683225","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
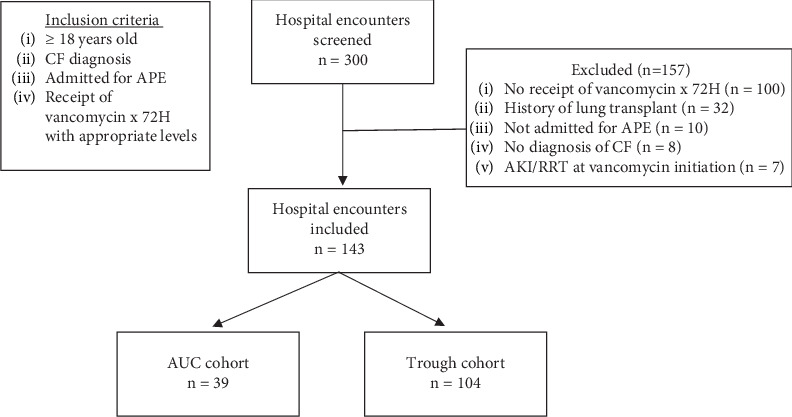
Background: Therapeutic drug monitoring (TDM) for vancomycin (VAN) in adult people with cystic fibrosis (pwCF) historically has utilized trough concentrations. Recent VAN TDM guidelines recommend area under the curve (AUC) monitoring to reduce the risk of acute kidney injury (AKI), despite limited evidence to support this practice in adult pwCF. Methods: This single-center, retrospective, observational cohort study included 143 adult pwCF admitted from July 1, 2017, to July 1, 2022, with an acute pulmonary exacerbation that received VAN for at least 72 h with available VAN plasma concentrations for TDM for AUC (n = 39) or trough monitoring (n = 104). Eligible patients with multiple hospital admissions during the study period were incorporated as separate encounters. The primary outcome was the incidence of AKI. Results: Receipt of concurrent nephrotoxins was more common in the AUC cohort than in the trough cohort (97% vs. 81%, p = 0.01), but the rate of AKI was similar (7.7% vs. 10.6%, p = 0.76). AUC monitoring was associated with earlier achievement of TDM goal (median 0 days (IQR 0-2) vs. 2 days (IQR 0-4), p < 0.01), lower total daily doses (34.8 mg/kg/day (IQR 27.6-49) vs. 57.5 mg/kg/day (IQR 43.9-68.6), p < 0.01), and fewer regimen changes (median 1 change (IQR 0-2) vs. 2 changes (IQR 1-3), p < 0.01). In patients with MRSA, pulmonary function recovery, readmission, and mortality were similar. Conclusion: In adult pwCF, the incidence of AKI was similar between AUC and trough monitoring cohorts; however, AUC monitoring achieved therapeutic targets sooner with fewer regimen modifications without significantly increasing the number of concentrations compared to trough monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


