Alina Hua, Blanca Domenech-Ximenos, Begona Lopez, Giovanni Sanna, Amedeo Chiribiri, Ronak Rajani, Michael Marber, David D'Cruz, Michelle Fernando, Tevfik F Ismail
{"title":"Diagnostic utility of the revised Lake Louise criteria in myocarditis associated with active autoimmune rheumatic disease.","authors":"Alina Hua, Blanca Domenech-Ximenos, Begona Lopez, Giovanni Sanna, Amedeo Chiribiri, Ronak Rajani, Michael Marber, David D'Cruz, Michelle Fernando, Tevfik F Ismail","doi":"10.1016/j.jocmr.2025.101916","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular magnetic resonance (CMR) is the principal non-invasive imaging modality used to diagnose idiopathic/viral myocarditis. The revised Lake Louise criteria (LLC) stipulate that a diagnosis can be made in the presence of one T1-based and one T2-based criterion. While the LLC have been extensively validated in viral myocarditis, their utility for the diagnosis of myocarditis due to an active autoimmune rheumatic disease is unknown. This study sought to assess the performance of the revised LLC in patients with clinically suspected myocarditis due to active systemic autoimmune disease.</p><p><strong>Methods: </strong>Patients with clinically active autoimmune rheumatic disease, symptoms of myocarditis, and elevated troponin levels were recruited and compared with controls with autoimmune rheumatic disease but no suspicion of autoimmune myocarditis. All patients underwent CMR at 1.5T including T1 and T2 mapping.</p><p><strong>Results: </strong>Thirty-seven patients with suspected myocarditis due to an active autoimmune rheumatic disease were recruited with a median (interquartile [IQR]) troponin level of 121 ng/L (72-318 ng/L). Overall, 65% (24/37) of patients met either of the two revised LLC resulting in a sensitivity (95% confidence interval) of 65% (49-78%) and specificity of 76% (57-89%). Only 32% (12/37) of patients fulfilled both of the main LLC (i.e., non-ischemic myocardial injury/edema with elevated T1 values or presence of late gadolinium enhancement and myocardial edema detected by increased T2 values or positive T2-STIR), resulting in a sensitivity of 32% (20-49%) and specificity of 100% (87-100%). Among controls, 24% (6/25) of patients had elevated native T1 values, but all had normal T2.</p><p><strong>Conclusion: </strong>In patients with suspected myocarditis due to autoimmune rheumatic disease, who are receiving immunosuppressive therapy, the LLC have a high specificity, but a lower sensitivity than in patients with viral myocarditis. Additional tests should therefore be used to improve disease detection in this population. Where the pre-test probability is high, in patients with suspected myocarditis due to autoimmune rheumatic disease who are undergoing immunosuppression, there may need to be greater reliance on one T1-based criterion rather than both LLC, with the recognition that there is an appreciable rate of raised T1 in controls without myocarditis.</p>","PeriodicalId":15221,"journal":{"name":"Journal of Cardiovascular Magnetic Resonance","volume":" ","pages":"101916"},"PeriodicalIF":6.1000,"publicationDate":"2025-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445391/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Magnetic Resonance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jocmr.2025.101916","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiovascular magnetic resonance (CMR) is the principal non-invasive imaging modality used to diagnose idiopathic/viral myocarditis. The revised Lake Louise criteria (LLC) stipulate that a diagnosis can be made in the presence of one T1-based and one T2-based criterion. While the LLC have been extensively validated in viral myocarditis, their utility for the diagnosis of myocarditis due to an active autoimmune rheumatic disease is unknown. This study sought to assess the performance of the revised LLC in patients with clinically suspected myocarditis due to active systemic autoimmune disease.
Methods: Patients with clinically active autoimmune rheumatic disease, symptoms of myocarditis, and elevated troponin levels were recruited and compared with controls with autoimmune rheumatic disease but no suspicion of autoimmune myocarditis. All patients underwent CMR at 1.5T including T1 and T2 mapping.
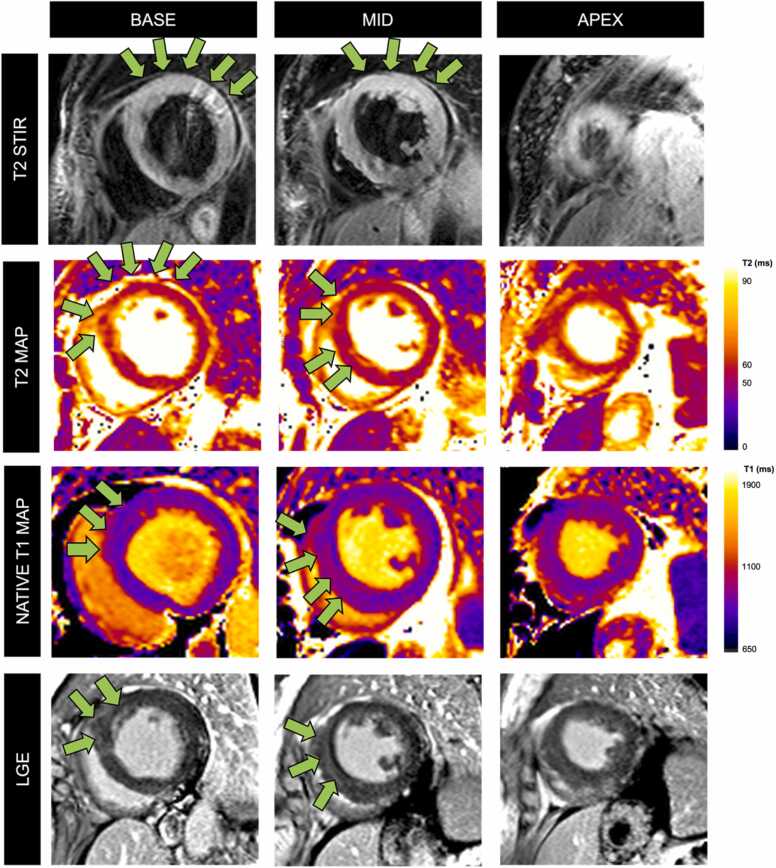
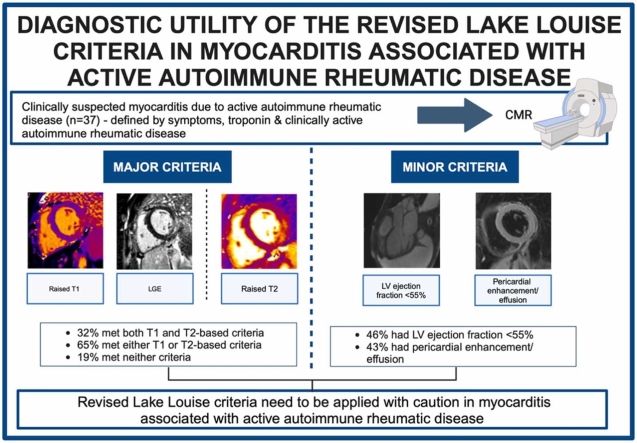
Results: Thirty-seven patients with suspected myocarditis due to an active autoimmune rheumatic disease were recruited with a median (interquartile [IQR]) troponin level of 121 ng/L (72-318 ng/L). Overall, 65% (24/37) of patients met either of the two revised LLC resulting in a sensitivity (95% confidence interval) of 65% (49-78%) and specificity of 76% (57-89%). Only 32% (12/37) of patients fulfilled both of the main LLC (i.e., non-ischemic myocardial injury/edema with elevated T1 values or presence of late gadolinium enhancement and myocardial edema detected by increased T2 values or positive T2-STIR), resulting in a sensitivity of 32% (20-49%) and specificity of 100% (87-100%). Among controls, 24% (6/25) of patients had elevated native T1 values, but all had normal T2.
Conclusion: In patients with suspected myocarditis due to autoimmune rheumatic disease, who are receiving immunosuppressive therapy, the LLC have a high specificity, but a lower sensitivity than in patients with viral myocarditis. Additional tests should therefore be used to improve disease detection in this population. Where the pre-test probability is high, in patients with suspected myocarditis due to autoimmune rheumatic disease who are undergoing immunosuppression, there may need to be greater reliance on one T1-based criterion rather than both LLC, with the recognition that there is an appreciable rate of raised T1 in controls without myocarditis.
期刊介绍:
Journal of Cardiovascular Magnetic Resonance (JCMR) publishes high-quality articles on all aspects of basic, translational and clinical research on the design, development, manufacture, and evaluation of cardiovascular magnetic resonance (CMR) methods applied to the cardiovascular system. Topical areas include, but are not limited to:
New applications of magnetic resonance to improve the diagnostic strategies, risk stratification, characterization and management of diseases affecting the cardiovascular system.
New methods to enhance or accelerate image acquisition and data analysis.
Results of multicenter, or larger single-center studies that provide insight into the utility of CMR.
Basic biological perceptions derived by CMR methods.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


