{"title":"Intensive care infection score: ICIS discriminates between infected and uninfected critically ill patients in routine intensive care unit practice.","authors":"Emre Deniz, Stefanie Klatte, Nilgün Tekin-Bubenheim, Mathias Zimmermann","doi":"10.1186/s40635-025-00767-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diagnosis of infectious inflammation is challenging as acute phase protein expression is nonspecific, limiting the utility of well-established biomarkers, such as procalcitonin (PCT) and C-reactive protein (CRP). The emergent blood cell-derived Intensive Care Infection Score (ICIS) is an innovative approach for the sensitive and specific diagnosis of infection in intensive care unit (ICU) patients. This study aimed to confirm the suitability of routine ICIS use in various ICU settings.</p><p><strong>Methods: </strong>This retrospective study included 115 patients from three ICUs. Seventy-five patients were diagnosed as infected and 40 as uninfected. ICIS, CRP, and PCT were compared to routine clinical assessment to evaluate their effectiveness in predicting infection in critically ill patients.</p><p><strong>Results: </strong>ICIS was superior to CRP and PCT in discriminating infection from no infection on day 1 in the ICU. In receiver operating characteristic curve analysis, ICIS exhibited an AUC = 0.984, sensitivity of 90.7%, specificity of 97.5%, positive predictive value (PPV) of 97.7% and negative predictive value (NPV) of 89.9%, by the best cutoff value of 3. CRP gave an AUC = 0.727, PPV of 70.0% and NPV of 67.8% by best cutoff value of 8.3 mg/L with a sensitivity of 74.7% and specificity of 62.5%. The best cutoff value of 0.9 ng/mL was calculated for PCT with an AUC = 0.812, PPV of 84.4%, NPV of 70.3%, sensitivity of 69.3% and specificity of 85.0%.</p><p><strong>Conclusions: </strong>ICIS outperformed CRP and PCT in identifying infection in critically ill patients across different ICU settings on the first day in the ICU. The high NPV emphasizes the potential of ICIS as an adjuvant tool to rule out infections thereby facilitating the reduction of antibiotic overuse and consequently limiting antimicrobial resistance (AMR) development. ICIS appears suitable for routine implementation in various ICU settings.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"58"},"PeriodicalIF":2.8000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12141177/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00767-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
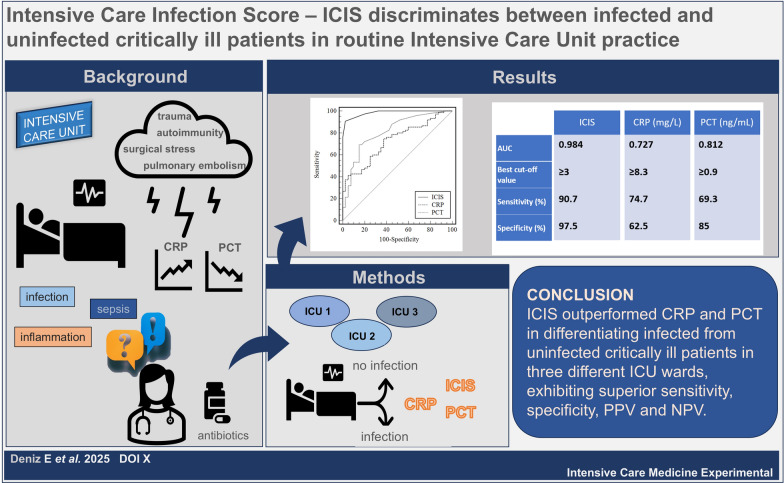
Background: Diagnosis of infectious inflammation is challenging as acute phase protein expression is nonspecific, limiting the utility of well-established biomarkers, such as procalcitonin (PCT) and C-reactive protein (CRP). The emergent blood cell-derived Intensive Care Infection Score (ICIS) is an innovative approach for the sensitive and specific diagnosis of infection in intensive care unit (ICU) patients. This study aimed to confirm the suitability of routine ICIS use in various ICU settings.
Methods: This retrospective study included 115 patients from three ICUs. Seventy-five patients were diagnosed as infected and 40 as uninfected. ICIS, CRP, and PCT were compared to routine clinical assessment to evaluate their effectiveness in predicting infection in critically ill patients.
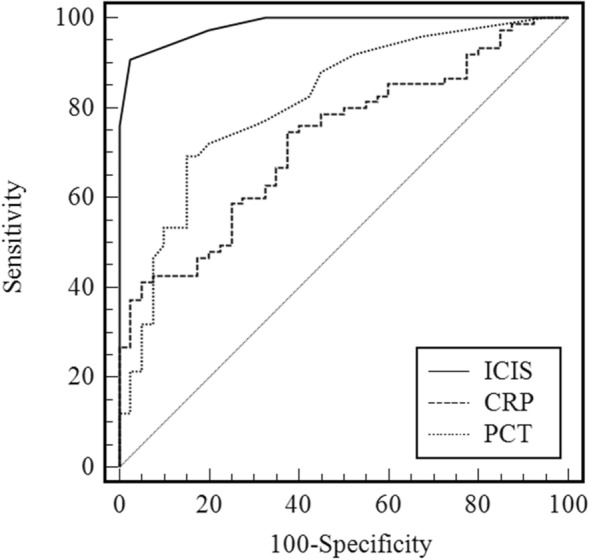
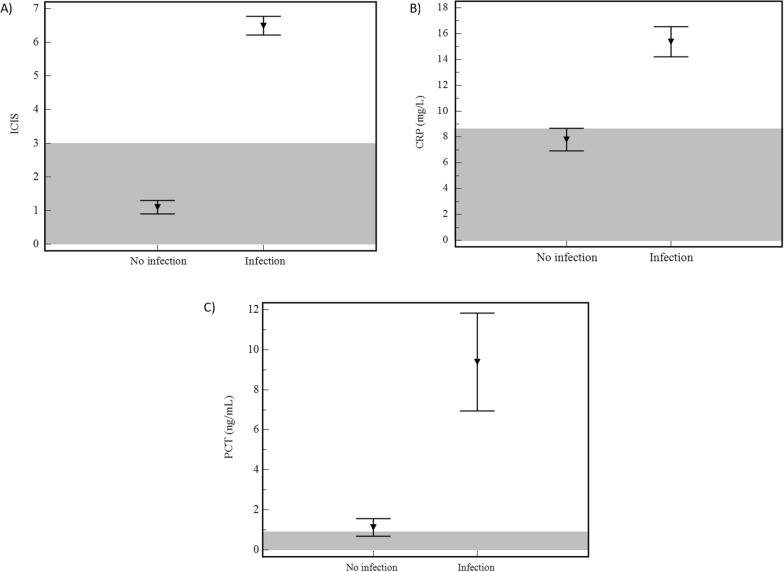
Results: ICIS was superior to CRP and PCT in discriminating infection from no infection on day 1 in the ICU. In receiver operating characteristic curve analysis, ICIS exhibited an AUC = 0.984, sensitivity of 90.7%, specificity of 97.5%, positive predictive value (PPV) of 97.7% and negative predictive value (NPV) of 89.9%, by the best cutoff value of 3. CRP gave an AUC = 0.727, PPV of 70.0% and NPV of 67.8% by best cutoff value of 8.3 mg/L with a sensitivity of 74.7% and specificity of 62.5%. The best cutoff value of 0.9 ng/mL was calculated for PCT with an AUC = 0.812, PPV of 84.4%, NPV of 70.3%, sensitivity of 69.3% and specificity of 85.0%.
Conclusions: ICIS outperformed CRP and PCT in identifying infection in critically ill patients across different ICU settings on the first day in the ICU. The high NPV emphasizes the potential of ICIS as an adjuvant tool to rule out infections thereby facilitating the reduction of antibiotic overuse and consequently limiting antimicrobial resistance (AMR) development. ICIS appears suitable for routine implementation in various ICU settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


