Phillip Scheinberg, Matt R Khoshnevis, Philip A Robinson, Alfredo Guerreros, Victor A H Sato, Benedito A L Fonseca, Hans W Prozesky, José Omar Chacón Romero, Laura Fogliatto, Barry R Meisenberg, David J Park, Ashok Gupta, Priti Patel, Danielle M Townsley, Lianqing Zheng, Veerendra Munugalavadla
{"title":"Efficacy and safety of acalabrutinib with best supportive care versus best supportive care in patients with COVID-19 requiring hospitalization.","authors":"Phillip Scheinberg, Matt R Khoshnevis, Philip A Robinson, Alfredo Guerreros, Victor A H Sato, Benedito A L Fonseca, Hans W Prozesky, José Omar Chacón Romero, Laura Fogliatto, Barry R Meisenberg, David J Park, Ashok Gupta, Priti Patel, Danielle M Townsley, Lianqing Zheng, Veerendra Munugalavadla","doi":"10.1093/immhor/vlaf023","DOIUrl":null,"url":null,"abstract":"<p><p>The efficacy and safety of acalabrutinib, a Bruton tyrosine kinase (BTK) inhibitor, was evaluated in 2 phase 2 studies in hospitalized patients with coronavirus disease 2019 (COVID-19) who received acalabrutinib + best supportive care (BSC) versus BSC alone (Clinicaltrials.gov: NCT04380688 and NCT04346199). The primary endpoint was the percentage of patients alive and free of respiratory failure on day 14 (rest of the world [RoW] study) and day 28 (US study). In the RoW study, 177 patients were randomized (acalabrutinib + BSC: n = 89; BSC: n = 88); in the US study, 62 patients were randomized (acalabrutinib + BSC: n = 31; BSC: n = 31). The percentage of patients who met the primary endpoint was similar in both studies (RoW study: acalabrutinib + BSC: 83.1%, BSC: 90.9%; US study: acalabrutinib + BSC: 80.6%, BSC: 83.9%). No new safety concerns were reported. Overall, no significant clinical benefit of adding acalabrutinib to BSC in patients hospitalized with COVID-19 was observed.</p>","PeriodicalId":94037,"journal":{"name":"ImmunoHorizons","volume":"9 7","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12133263/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ImmunoHorizons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/immhor/vlaf023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
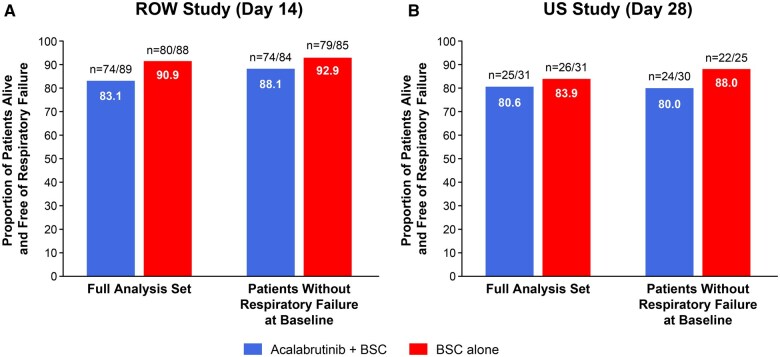
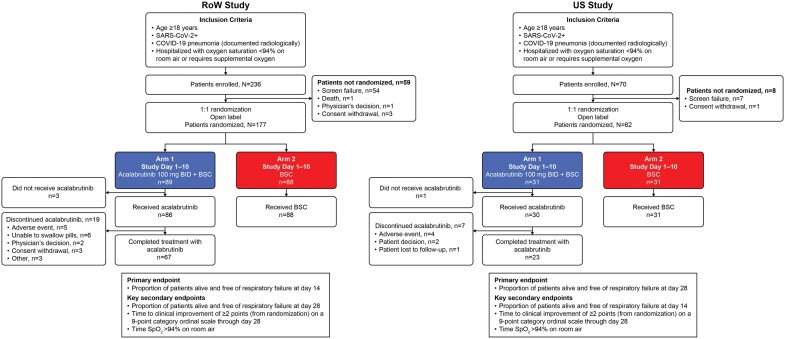
The efficacy and safety of acalabrutinib, a Bruton tyrosine kinase (BTK) inhibitor, was evaluated in 2 phase 2 studies in hospitalized patients with coronavirus disease 2019 (COVID-19) who received acalabrutinib + best supportive care (BSC) versus BSC alone (Clinicaltrials.gov: NCT04380688 and NCT04346199). The primary endpoint was the percentage of patients alive and free of respiratory failure on day 14 (rest of the world [RoW] study) and day 28 (US study). In the RoW study, 177 patients were randomized (acalabrutinib + BSC: n = 89; BSC: n = 88); in the US study, 62 patients were randomized (acalabrutinib + BSC: n = 31; BSC: n = 31). The percentage of patients who met the primary endpoint was similar in both studies (RoW study: acalabrutinib + BSC: 83.1%, BSC: 90.9%; US study: acalabrutinib + BSC: 80.6%, BSC: 83.9%). No new safety concerns were reported. Overall, no significant clinical benefit of adding acalabrutinib to BSC in patients hospitalized with COVID-19 was observed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


