Ananya Shah, Adam M Carroll, Nicolas Chanes, Kyndall Hadley, Cenea Kemp, Bo Chang Brian Wu, Alejandro Suarez-Pierre, Jessica Rove, Catherine Velopulos, Muhammad Aftab, T Brett Reece
{"title":"Evaluating Patient Outcomes and Access to Care in Aortic Surgery Based on Ethnicity and Social Vulnerability.","authors":"Ananya Shah, Adam M Carroll, Nicolas Chanes, Kyndall Hadley, Cenea Kemp, Bo Chang Brian Wu, Alejandro Suarez-Pierre, Jessica Rove, Catherine Velopulos, Muhammad Aftab, T Brett Reece","doi":"10.1055/a-2608-1346","DOIUrl":null,"url":null,"abstract":"<p><p>We previously demonstrated the impact of ethnicity on aortic surgery, with underrepresentation and greater acuity in minority patients, raising concerns regarding access to care. The Centers for Disease Control and Prevention's social vulnerability index (SVI) measure is increasingly used to quantify patient socioeconomic and demographic factors. This study expands on our prior work by incorporating SVI and ethnicity to analyze patient presentation and outcomes in aortic arch surgery.We utilized a single-institution database of patients who underwent total arch replacement or hemiarch repair between 2009 and 2022. A total of 837 patients were placed into five cohorts based on their self-reported race: African American, Asian, Caucasian, Hispanic, and Other, with further subdivision based on SVI (high social vulnerability, ≥75%, normal social vulnerability < 75%). Additional analyses were performed using SVI alone. We compared patient presentation, operative variables, and outcomes based on the above cohorts.African American and Hispanic patients were underrepresented compared with city demographics. High SVI and minority patients presented at younger ages (<i>p</i> = 0.007) with higher blood pressures (<i>p</i> = 0.002). These groups also had more urgent/emergent presentations (<i>p</i> < 0.001) with aortic dissections (<i>p</i> = 0.006). Operatively, high SVI groups had longer cardiopulmonary bypass (<i>p</i> = 0.018), cross-clamp (<i>p</i> = 0.020), and circulatory arrest times (<i>p</i> = 0.002) but fewer adjunctive procedures (<i>p</i> = 0.018). High SVI patients more often required total arch replacement (<i>p</i> = 0.048) and postoperative mechanical circulatory support (<i>p</i> = 0.025). After discharge, African Americans had more emergency department (ED) visits within a year (<i>p</i> < 0.001), although no significant differences were observed in readmission rates or cardiovascular follow-up.Underrepresented groups face barriers to care, as reflected in disparities in demographics, surgical acuity, and postdischarge ED usage. Analyses-based solely on ethnicity overlooked critical differences between normal and high SVI groups, emphasizing the need for care strategies that are both tailored to high SVI groups and racially sensitive applied across all levels of health care.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"29-38"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202025/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2608-1346","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
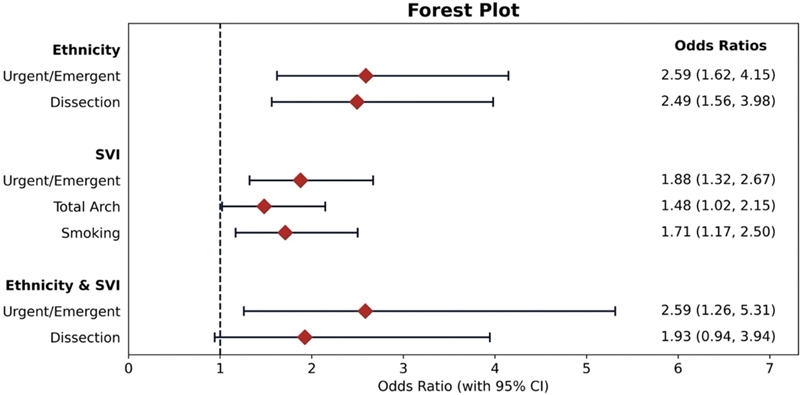
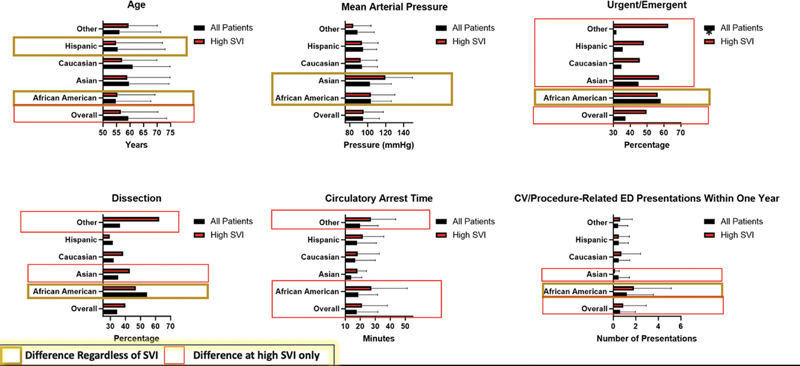
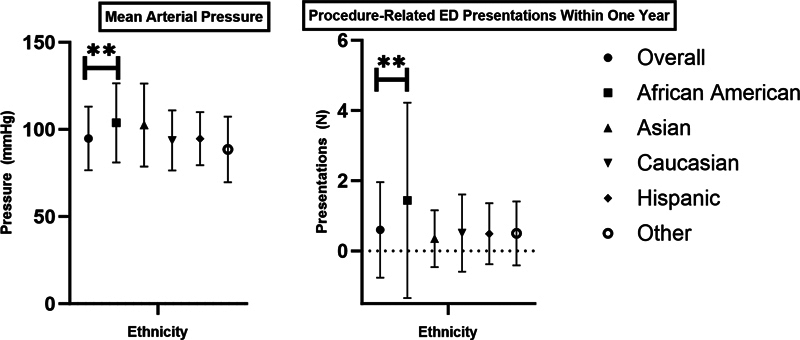
We previously demonstrated the impact of ethnicity on aortic surgery, with underrepresentation and greater acuity in minority patients, raising concerns regarding access to care. The Centers for Disease Control and Prevention's social vulnerability index (SVI) measure is increasingly used to quantify patient socioeconomic and demographic factors. This study expands on our prior work by incorporating SVI and ethnicity to analyze patient presentation and outcomes in aortic arch surgery.We utilized a single-institution database of patients who underwent total arch replacement or hemiarch repair between 2009 and 2022. A total of 837 patients were placed into five cohorts based on their self-reported race: African American, Asian, Caucasian, Hispanic, and Other, with further subdivision based on SVI (high social vulnerability, ≥75%, normal social vulnerability < 75%). Additional analyses were performed using SVI alone. We compared patient presentation, operative variables, and outcomes based on the above cohorts.African American and Hispanic patients were underrepresented compared with city demographics. High SVI and minority patients presented at younger ages (p = 0.007) with higher blood pressures (p = 0.002). These groups also had more urgent/emergent presentations (p < 0.001) with aortic dissections (p = 0.006). Operatively, high SVI groups had longer cardiopulmonary bypass (p = 0.018), cross-clamp (p = 0.020), and circulatory arrest times (p = 0.002) but fewer adjunctive procedures (p = 0.018). High SVI patients more often required total arch replacement (p = 0.048) and postoperative mechanical circulatory support (p = 0.025). After discharge, African Americans had more emergency department (ED) visits within a year (p < 0.001), although no significant differences were observed in readmission rates or cardiovascular follow-up.Underrepresented groups face barriers to care, as reflected in disparities in demographics, surgical acuity, and postdischarge ED usage. Analyses-based solely on ethnicity overlooked critical differences between normal and high SVI groups, emphasizing the need for care strategies that are both tailored to high SVI groups and racially sensitive applied across all levels of health care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


