Shifeng Feng, Ou Huiying, Guo Wei, Jingsheng Yuan, Tao Lv, Jian Yang, Yong Zhao, Lingxiang Kong, Jiayin Yang
{"title":"Influence of portal hypertension-associated upper gastrointestinal bleeding and acute kidney injury on liver transplantation prognosis.","authors":"Shifeng Feng, Ou Huiying, Guo Wei, Jingsheng Yuan, Tao Lv, Jian Yang, Yong Zhao, Lingxiang Kong, Jiayin Yang","doi":"10.1186/s13741-025-00545-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Given that prioritization for liver transplantation (LT) is based primarily on the model for end-stage liver disease (MELD) scores, patients with lower MELD scores, who experience chronic anemia and recurrent hypotension due to gastrointestinal bleeding (GIB), tend to be marginalized.</p><p><strong>Methods: </strong>A total of 581 patients with no evidence of acute kidney injury (AKI) or chronic kidney disease 2 months before LT constituted a retrospective cohort. Within this cohort, a nested case-control study was conducted that included 134 patients with preoperative GIB (GIB(+)) and 246 matched patients without preoperative GIB (GIB(-)). A subgroup analysis was conducted based on the occurrence of AKI (AKI(- /+)) within 2 months prior to LT.</p><p><strong>Results: </strong>The incidence of preoperative AKI was significantly higher in patients with GIB(+) compared with patients with GIB(-) (14.9% vs 8.1%, P=0.039), along with higher rates of postoperative complications and prolonged hospital stay; however, long-term survival rates were similar between the two groups. Subgroup analysis also revealed that the postoperative incidence of AKI and mortality rates at 60 days were elevated in patients with preoperative GIB(+) AKI(+) compared with patients with GIB(+) AKI(-). Furthermore, 5-year survival rates were significantly lower for patients with GIB(+) AKI(+) (65.0% vs 82.5%, P = 0.040). However, no significant difference was observed between the two subgroups of AKI(+) (GIB(+) versus GIB(-)) and the two subgroups of AKI(-) in relation to postoperative complications, short-term mortality, and long-term survival rates.</p><p><strong>Conclusions: </strong>Patients who experience preoperative GIB face an elevated risk of developing AKI, which is significantly correlated with a poorer prognosis for LT. A more proactive approach is needed to assess the transplant priority of patients with GIB on the waiting list.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"14 1","pages":"61"},"PeriodicalIF":2.1000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12131653/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-025-00545-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Given that prioritization for liver transplantation (LT) is based primarily on the model for end-stage liver disease (MELD) scores, patients with lower MELD scores, who experience chronic anemia and recurrent hypotension due to gastrointestinal bleeding (GIB), tend to be marginalized.
Methods: A total of 581 patients with no evidence of acute kidney injury (AKI) or chronic kidney disease 2 months before LT constituted a retrospective cohort. Within this cohort, a nested case-control study was conducted that included 134 patients with preoperative GIB (GIB(+)) and 246 matched patients without preoperative GIB (GIB(-)). A subgroup analysis was conducted based on the occurrence of AKI (AKI(- /+)) within 2 months prior to LT.
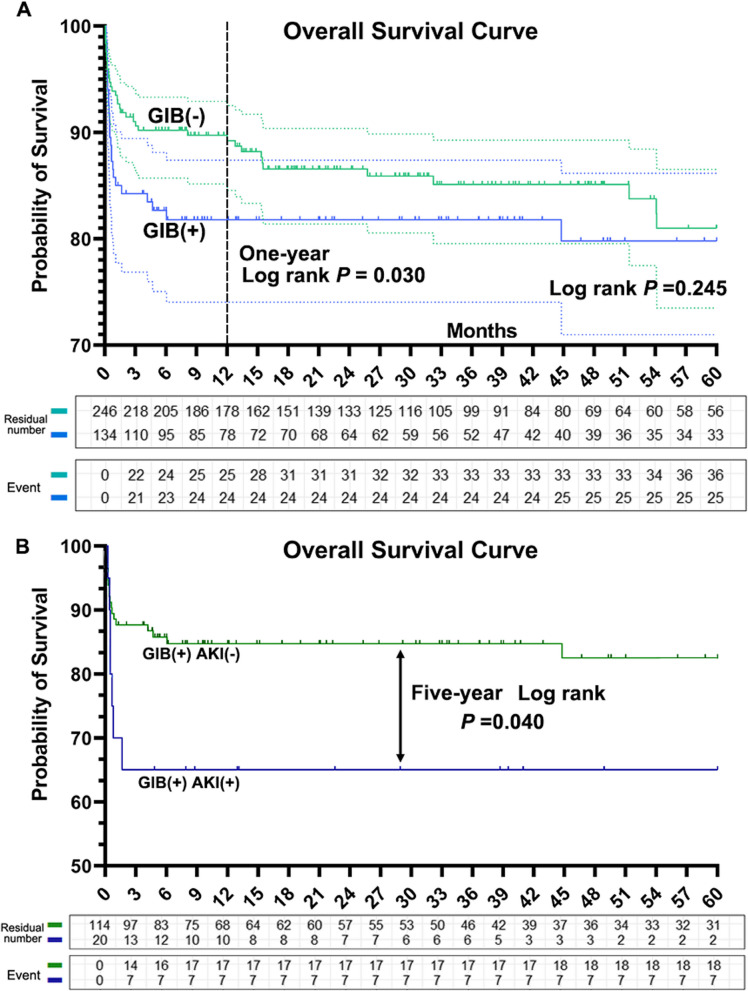
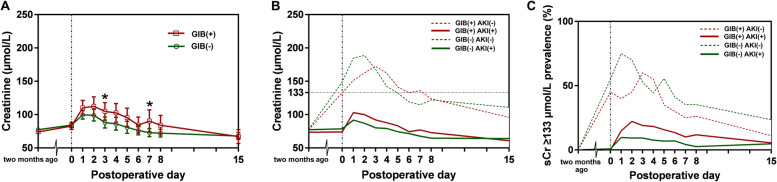
Results: The incidence of preoperative AKI was significantly higher in patients with GIB(+) compared with patients with GIB(-) (14.9% vs 8.1%, P=0.039), along with higher rates of postoperative complications and prolonged hospital stay; however, long-term survival rates were similar between the two groups. Subgroup analysis also revealed that the postoperative incidence of AKI and mortality rates at 60 days were elevated in patients with preoperative GIB(+) AKI(+) compared with patients with GIB(+) AKI(-). Furthermore, 5-year survival rates were significantly lower for patients with GIB(+) AKI(+) (65.0% vs 82.5%, P = 0.040). However, no significant difference was observed between the two subgroups of AKI(+) (GIB(+) versus GIB(-)) and the two subgroups of AKI(-) in relation to postoperative complications, short-term mortality, and long-term survival rates.
Conclusions: Patients who experience preoperative GIB face an elevated risk of developing AKI, which is significantly correlated with a poorer prognosis for LT. A more proactive approach is needed to assess the transplant priority of patients with GIB on the waiting list.
背景:考虑到肝移植(LT)的优先级主要基于终末期肝病(MELD)评分模型,MELD评分较低的患者,由于胃肠道出血(GIB)而经历慢性贫血和复发性低血压,往往被边缘化。方法:581例在肝移植前2个月无急性肾损伤(AKI)或慢性肾脏疾病的患者组成回顾性队列。在该队列中,进行了一项巢式病例对照研究,包括134例术前GIB患者(GIB(+))和246例术前无GIB患者(GIB(-))。基于lt前2个月内AKI(AKI(- /+))的发生率进行亚组分析。结果:GIB(+)患者术前AKI发生率明显高于GIB(-)患者(14.9% vs 8.1%, P=0.039),同时术后并发症发生率和住院时间延长;然而,两组的长期存活率是相似的。亚组分析还显示,术前GIB(+) AKI(+)患者术后AKI发生率和60天死亡率高于术前GIB(+) AKI(-)患者。此外,GIB(+) AKI(+)患者的5年生存率显著降低(65.0% vs 82.5%, P = 0.040)。然而,AKI(+)的两个亚组(GIB(+)与GIB(-))和AKI(-)的两个亚组在术后并发症、短期死亡率和长期生存率方面没有显著差异。结论:术前经历GIB的患者发生AKI的风险升高,这与lt预后较差显著相关。需要更积极的方法来评估等待名单上GIB患者的移植优先级。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


