Diagnostic performance of cardiovascular magnetic resonance parametric mapping as per modified Lake Louise Criteria in acute myocarditis: an updated systematic review and meta-analysis.
Latika Giri, Roshan Singh, Ahmed Marey, Yupeng Li, Bharath Ambale Venkatesh, Jawdat Abdulla, Stefan Zimmerman, Muhammad Umair
{"title":"Diagnostic performance of cardiovascular magnetic resonance parametric mapping as per modified Lake Louise Criteria in acute myocarditis: an updated systematic review and meta-analysis.","authors":"Latika Giri, Roshan Singh, Ahmed Marey, Yupeng Li, Bharath Ambale Venkatesh, Jawdat Abdulla, Stefan Zimmerman, Muhammad Umair","doi":"10.1186/s44348-025-00048-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular magnetic resonance mapping parameters-native T1 mapping, T2 mapping, and extracellular volume (ECV)-are key for diagnosing acute myocarditis under the modified 2018 Lake Louise Criteria (mLLC). This systematic review and meta-analysis evaluated their diagnostic performance and established optimal thresholds for acute myocarditis.</p><p><strong>Methods: </strong>We reviewed articles published in the past decade utilizing parametric mapping for myocarditis diagnosis. Data on sensitivity, specificity, and area under the curve (AUC) were extracted. Quality assessment was conducted using the QUADAS-2 tool by two independent reviewers.</p><p><strong>Results: </strong>Eleven studies with 677 patients were included. Native T1 mapping showed sensitivity of 83%, specificity of 86%, diagnostic odds ratio (DOR) of 39, and an AUC of 0.91. T2 mapping had sensitivity of 81%, specificity of 86%, DOR of 25, and an AUC of 0.89. ECV demonstrated sensitivity of 71%, specificity of 81%, DOR of 13, and an AUC of 0.83. Mean control values were 1,039 ± 39.23 ms for native T1 mapping, 57 ± 5.18 ms for T2 mapping, and 31% ± 5.60% for ECV. Optimal thresholds were 1,021 ms for native T1 mapping, 52 ms for T2 mapping, and 28% for ECV based on receiver operating characteristic curves analysis based on 1.5-T scanner value. Native T1 mapping showed the highest diagnostic accuracy. Subgroup analysis found no significant sensitivity differences based on biopsy or clinical criteria.</p><p><strong>Conclusions: </strong>Parametric mapping, particularly native T1, demonstrated strong diagnostic performance for acute myocarditis compared to T2 mapping and ECV within the modified 2018 Lake Louise Criteria framework. Incorporating these cardiovascular magnetic resonance parameters may improve diagnostic accuracy. Further research is recommended to refine these findings and optimize diagnostic strategies.</p>","PeriodicalId":15229,"journal":{"name":"Journal of Cardiovascular Imaging","volume":"33 1","pages":"5"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12131415/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Imaging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44348-025-00048-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiovascular magnetic resonance mapping parameters-native T1 mapping, T2 mapping, and extracellular volume (ECV)-are key for diagnosing acute myocarditis under the modified 2018 Lake Louise Criteria (mLLC). This systematic review and meta-analysis evaluated their diagnostic performance and established optimal thresholds for acute myocarditis.
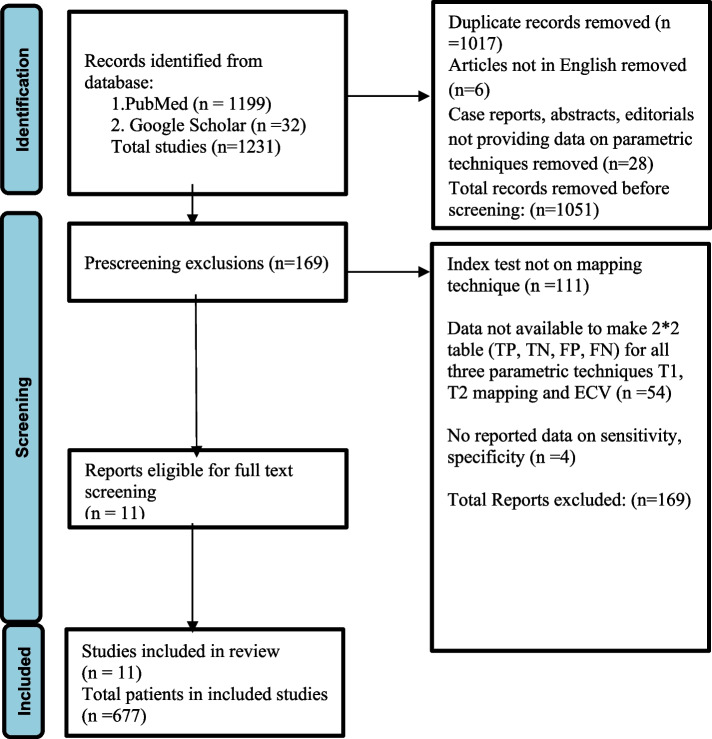
Methods: We reviewed articles published in the past decade utilizing parametric mapping for myocarditis diagnosis. Data on sensitivity, specificity, and area under the curve (AUC) were extracted. Quality assessment was conducted using the QUADAS-2 tool by two independent reviewers.
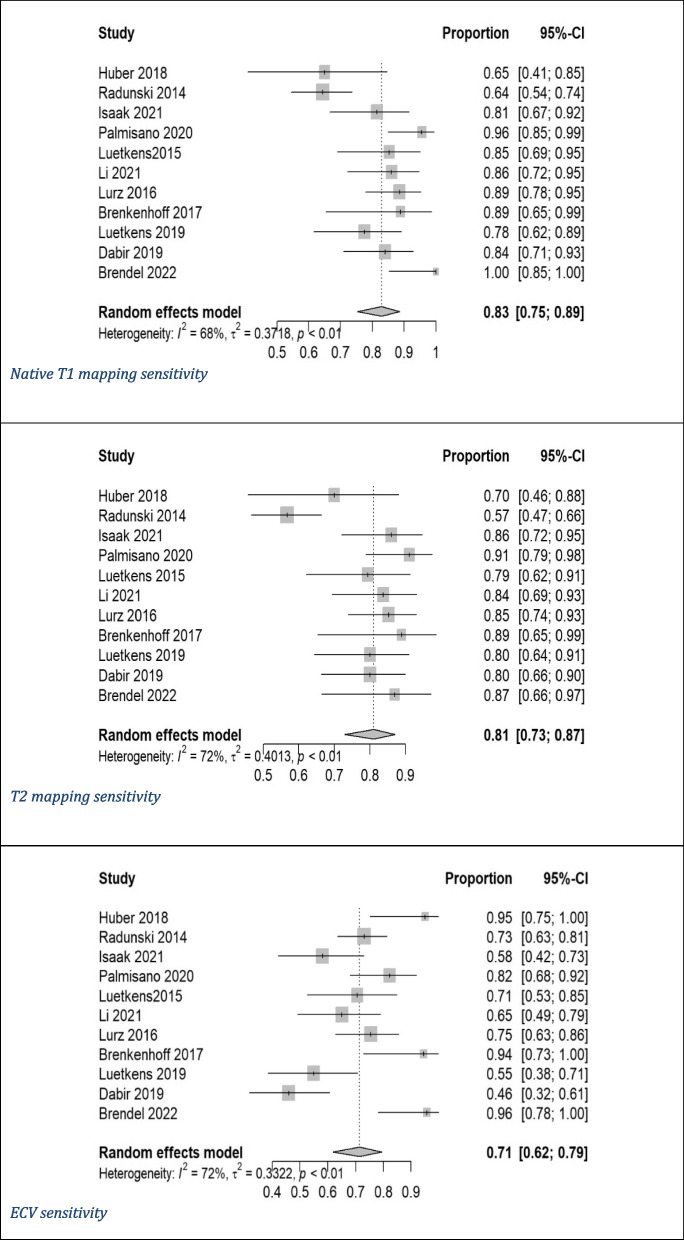
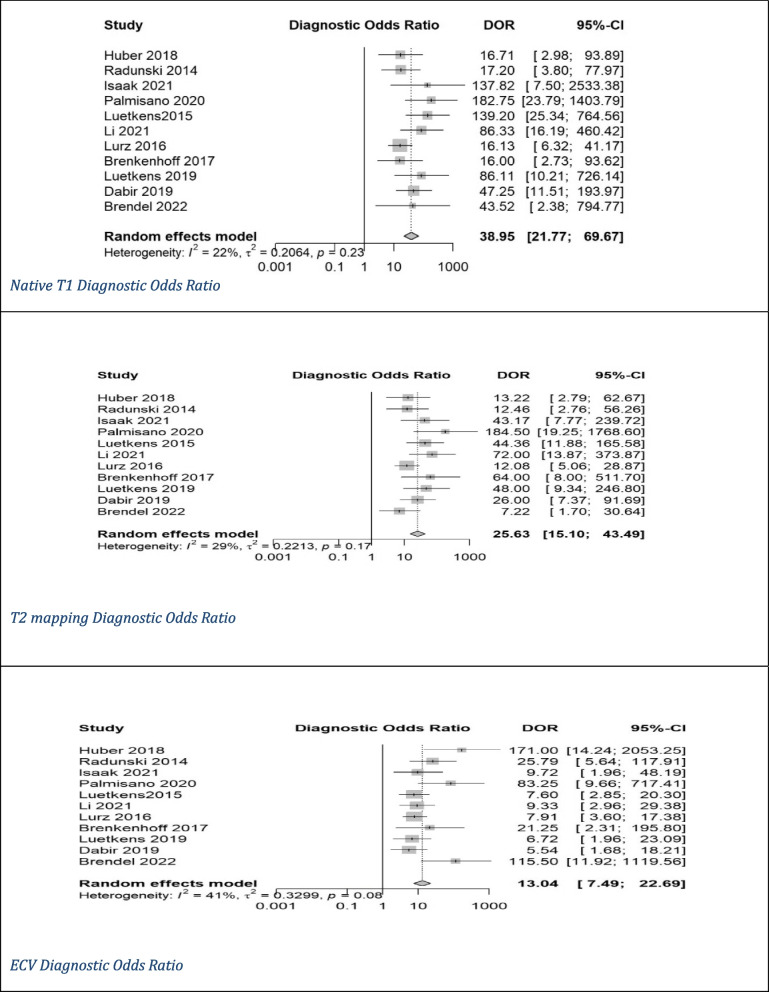
Results: Eleven studies with 677 patients were included. Native T1 mapping showed sensitivity of 83%, specificity of 86%, diagnostic odds ratio (DOR) of 39, and an AUC of 0.91. T2 mapping had sensitivity of 81%, specificity of 86%, DOR of 25, and an AUC of 0.89. ECV demonstrated sensitivity of 71%, specificity of 81%, DOR of 13, and an AUC of 0.83. Mean control values were 1,039 ± 39.23 ms for native T1 mapping, 57 ± 5.18 ms for T2 mapping, and 31% ± 5.60% for ECV. Optimal thresholds were 1,021 ms for native T1 mapping, 52 ms for T2 mapping, and 28% for ECV based on receiver operating characteristic curves analysis based on 1.5-T scanner value. Native T1 mapping showed the highest diagnostic accuracy. Subgroup analysis found no significant sensitivity differences based on biopsy or clinical criteria.
Conclusions: Parametric mapping, particularly native T1, demonstrated strong diagnostic performance for acute myocarditis compared to T2 mapping and ECV within the modified 2018 Lake Louise Criteria framework. Incorporating these cardiovascular magnetic resonance parameters may improve diagnostic accuracy. Further research is recommended to refine these findings and optimize diagnostic strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


