Amine Al Soueidy, Gregory Miller, Shawana Hussain, Jean-Sebastien Rachoin, Krystal Hunter, Elias Iliadis
{"title":"Aspiration thrombectomy compared to catheter directed thrombolysis in pulmonary embolism: Outcomes from a tertiary referral center.","authors":"Amine Al Soueidy, Gregory Miller, Shawana Hussain, Jean-Sebastien Rachoin, Krystal Hunter, Elias Iliadis","doi":"10.5603/cj.99047","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prompt treatment of pulmonary embolism (PE) prevents morbidity and mortality. The aim of the present study was to evaluate and compare the effectiveness of two FDA-approved catheter-based therapies (CBT) for acute PE: ultrasound-assisted catheter-directed thrombolysis EKOS (EKOS Corporation, Bothell, WA) and Penumbra Indigo aspiration thrombectomy (Penumbra Inc., Alameda, CA, USA).</p><p><strong>Methods: </strong>Patients with submassive and massive PE who underwent CBT between 09/2014 and 08/2022 at our institution were identified. Primary efficacy outcome was change in the echocardiographic RV/LV diameter ratio within 48 to 72h of the procedure.</p><p><strong>Results: </strong>A total of 189 patients underwent EKOS (n=119) or Penumbra (n = 70) for submassive (n = 175) and massive (n = 14) PE. The RV/LV ratio showed improvement post intervention, with 21.2% decrease in the EKOS group (EG) and 35.6% in the Penumbra group (PG). PG group had a greater reduction in RV/LV (median change 0.396 (IQR, 0.347) vs. 0.207 (IQR, 0.306), p < 0.001). The rate of complications and in-hospital mortality were similar (15.1% in EG and 10% in PG and 2.5% in EG, 4.3% in PG, p = 0.672; respectively). Subgroup analysis comparing responders, defined as patients with a post-intervention echocardiographic RV/LV ratio < 0.9, and non-responders showed a lower rate of chronic lung disease, (4.3% vs. 19.0%, p = 0.015).</p><p><strong>Conclusions: </strong>Both CBT options are promising for treating acute submassive or massive PE, with efficacy outcomes favoring aspiration thrombectomy. Presence of chronic lung disease was associated with lower response to CBT in terms of reversal of RV dysfunction. Longer follow-up and randomized controlled trials are needed for definitive conclusions.</p>","PeriodicalId":93923,"journal":{"name":"Cardiology journal","volume":" ","pages":"347-356"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12410932/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5603/cj.99047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/3 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prompt treatment of pulmonary embolism (PE) prevents morbidity and mortality. The aim of the present study was to evaluate and compare the effectiveness of two FDA-approved catheter-based therapies (CBT) for acute PE: ultrasound-assisted catheter-directed thrombolysis EKOS (EKOS Corporation, Bothell, WA) and Penumbra Indigo aspiration thrombectomy (Penumbra Inc., Alameda, CA, USA).
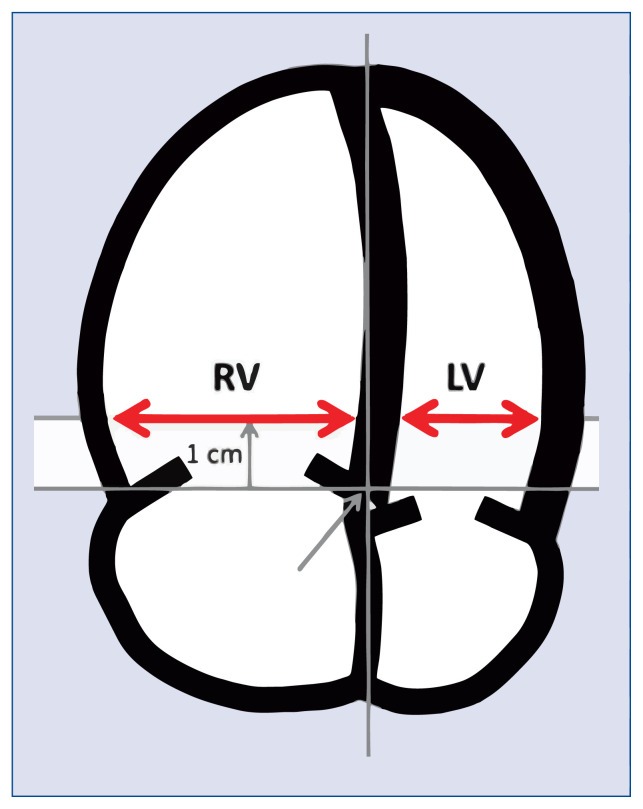
Methods: Patients with submassive and massive PE who underwent CBT between 09/2014 and 08/2022 at our institution were identified. Primary efficacy outcome was change in the echocardiographic RV/LV diameter ratio within 48 to 72h of the procedure.
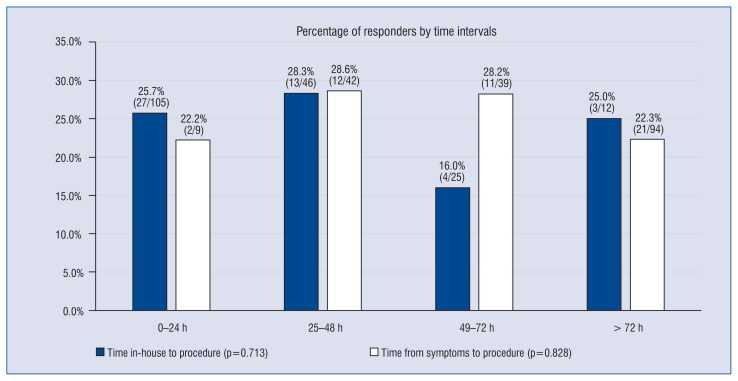
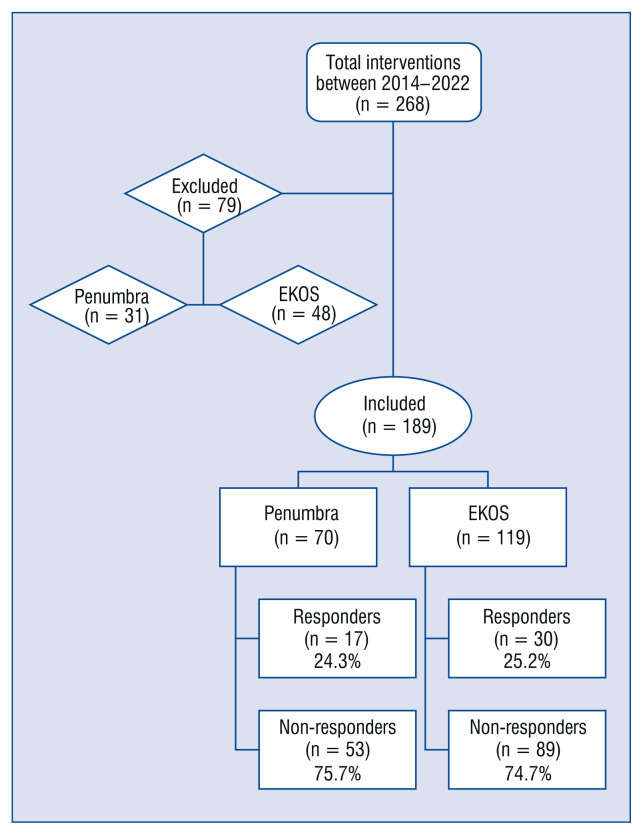
Results: A total of 189 patients underwent EKOS (n=119) or Penumbra (n = 70) for submassive (n = 175) and massive (n = 14) PE. The RV/LV ratio showed improvement post intervention, with 21.2% decrease in the EKOS group (EG) and 35.6% in the Penumbra group (PG). PG group had a greater reduction in RV/LV (median change 0.396 (IQR, 0.347) vs. 0.207 (IQR, 0.306), p < 0.001). The rate of complications and in-hospital mortality were similar (15.1% in EG and 10% in PG and 2.5% in EG, 4.3% in PG, p = 0.672; respectively). Subgroup analysis comparing responders, defined as patients with a post-intervention echocardiographic RV/LV ratio < 0.9, and non-responders showed a lower rate of chronic lung disease, (4.3% vs. 19.0%, p = 0.015).
Conclusions: Both CBT options are promising for treating acute submassive or massive PE, with efficacy outcomes favoring aspiration thrombectomy. Presence of chronic lung disease was associated with lower response to CBT in terms of reversal of RV dysfunction. Longer follow-up and randomized controlled trials are needed for definitive conclusions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


