12-Month Outcomes of a Prospective Randomized Trial Investigating Effects of IVIG on Top of rATG Versus rATG Alone in Pre-Sensitized Kidney Transplant Recipients: The INHIBIT Study.
Ondrej Viklicky, Ivan Zahradka, Jan Mares, Janka Slatinska, Alena Parikova, Vojtech Petr, Matej Roder, Katerina Jaklova, Klara Osickova, Libor Janousek, Petra Hruba
{"title":"12-Month Outcomes of a Prospective Randomized Trial Investigating Effects of IVIG on Top of rATG Versus rATG Alone in Pre-Sensitized Kidney Transplant Recipients: The INHIBIT Study.","authors":"Ondrej Viklicky, Ivan Zahradka, Jan Mares, Janka Slatinska, Alena Parikova, Vojtech Petr, Matej Roder, Katerina Jaklova, Klara Osickova, Libor Janousek, Petra Hruba","doi":"10.3389/ti.2025.14312","DOIUrl":null,"url":null,"abstract":"<p><p>Intravenous immunoglobulins (IVIG) are commonly used in peri-transplant desensitization, but evidence supporting their efficacy is limited. We conducted a prospective, randomized single-center, open-label, Phase IIIb non-inferiority clinical pilot trial to compare the efficacy of IVIG (administered at a dose of 3 × 0.5 g/kg) versus no IVIG, in conjunction with rabbit anti-thymocyte globulin (5-7 mg/kg) induction, in pre-sensitized patients with donor-specific antibodies who had negative pre-transplantation Flow- and CDC-crossmatches, between July 2020 and November 2022. The primary endpoint was the rate of efficacy failure, defined as biopsy-proven rejection within 12-month post-transplant. Secondary endpoints included the incidence of rejection at protocol biopsies, evaluated by histology and biopsy-based transcripts diagnostics. Of the screened patients, 53 (72.6%) were excluded due to crossmatch positivity. Ten patients were randomized to the IVIG+, and 7 to the IVIG-arm. The trial was prematurely terminated due to futility at interim analysis. In the IVIG-arm, 3 patients (43%) experienced the primary endpoint compared to none in the IVIG+ arm (p = 0.026). MMDx identified one molecular ABMR in the IVIG+ and 2 in the IVIG-arm in 12-month protocol biopsies. There was one graft loss in the IVIG-arm. The results of this pilot study, although not definitive, do not support the use of IVIG-sparing regimens in HLA-incompatible kidney transplantation (NCT04302805). This study is registered on ClinicalTrials.gov under the identifier NCT04302805.</p>","PeriodicalId":23343,"journal":{"name":"Transplant International","volume":"38 ","pages":"14312"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12127847/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/ti.2025.14312","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
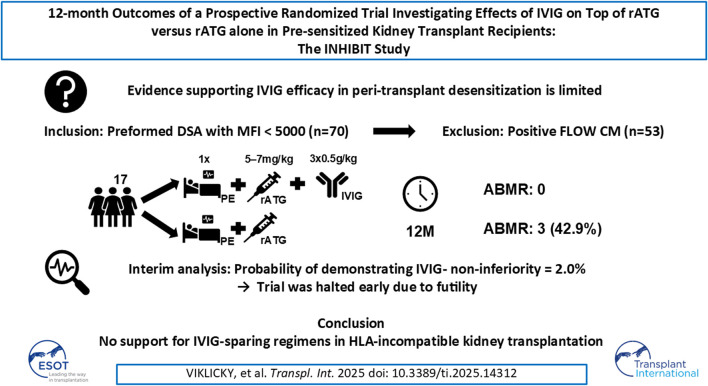
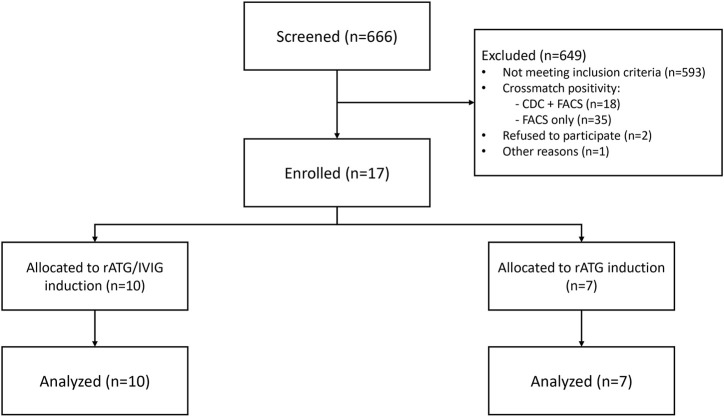
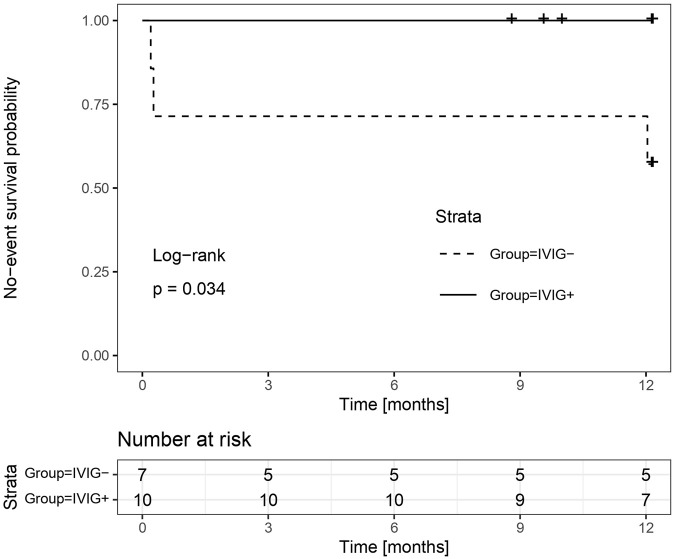
Intravenous immunoglobulins (IVIG) are commonly used in peri-transplant desensitization, but evidence supporting their efficacy is limited. We conducted a prospective, randomized single-center, open-label, Phase IIIb non-inferiority clinical pilot trial to compare the efficacy of IVIG (administered at a dose of 3 × 0.5 g/kg) versus no IVIG, in conjunction with rabbit anti-thymocyte globulin (5-7 mg/kg) induction, in pre-sensitized patients with donor-specific antibodies who had negative pre-transplantation Flow- and CDC-crossmatches, between July 2020 and November 2022. The primary endpoint was the rate of efficacy failure, defined as biopsy-proven rejection within 12-month post-transplant. Secondary endpoints included the incidence of rejection at protocol biopsies, evaluated by histology and biopsy-based transcripts diagnostics. Of the screened patients, 53 (72.6%) were excluded due to crossmatch positivity. Ten patients were randomized to the IVIG+, and 7 to the IVIG-arm. The trial was prematurely terminated due to futility at interim analysis. In the IVIG-arm, 3 patients (43%) experienced the primary endpoint compared to none in the IVIG+ arm (p = 0.026). MMDx identified one molecular ABMR in the IVIG+ and 2 in the IVIG-arm in 12-month protocol biopsies. There was one graft loss in the IVIG-arm. The results of this pilot study, although not definitive, do not support the use of IVIG-sparing regimens in HLA-incompatible kidney transplantation (NCT04302805). This study is registered on ClinicalTrials.gov under the identifier NCT04302805.
期刊介绍:
The aim of the journal is to serve as a forum for the exchange of scientific information in the form of original and high quality papers in the field of transplantation. Clinical and experimental studies, as well as editorials, letters to the editors, and, occasionally, reviews on the biology, physiology, and immunology of transplantation of tissues and organs, are published. Publishing time for the latter is approximately six months, provided major revisions are not needed. The journal is published in yearly volumes, each volume containing twelve issues. Papers submitted to the journal are subject to peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


