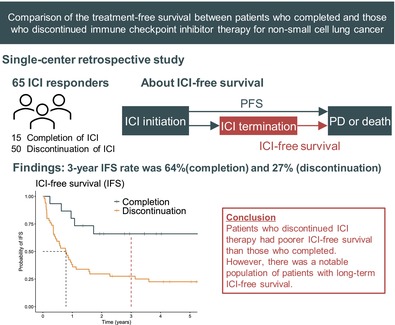
Comparison of the Immune Checkpoint InhibitorFree Survival Between Patients Who Completed and Those Who Discontinued ICI for Non-Small Cell Lung Cancer.
{"title":"Comparison of the Immune Checkpoint InhibitorFree Survival Between Patients Who Completed and Those Who Discontinued ICI for Non-Small Cell Lung Cancer.","authors":"Takahiro Nagai, Hiroaki Akamatsu, Eri Takase, Eriko Murakami, Takeya Sugimoto, Ryota Shibaki, Atsushi Hayata, Toshio Shimizu, Masanori Nakanishi, Yasuhiro Koh, Nobuyuki Yamamoto","doi":"10.1111/1759-7714.70090","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune checkpoint inhibitors (ICI)-containing therapy for advanced or recurrent non-small cell lung cancer (NSCLC) are not completed by some responders for reasons other than progressive disease (PD). The proportion of patients who discontinue ICI and the length of their treatment-free status are unclear.</p><p><strong>Methods: </strong>In this single-center retrospective study, we examined the medical records of 233 patients who initiated ICI-based therapy at our hospital between 2016 and 2020. We identified patients who completed treatment and discontinued it for reasons other than PD. The primary outcome was treatment-free survival, which we termed ICI-free survival.</p><p><strong>Results: </strong>Sixty-five patients were eligible for analysis. In the discontinuation group, the median duration of ICI was 3.9 months. Median progression-free survival, ICI-free survival, and overall survival in the entire population were 25.0, 11.5, and 78.3 months, respectively. The ICI-free survival rates at 1, 2, and 3 years were 48%, 38%, and 36%. The Kaplan-Meier curve of ICI-free survival almost reached a plateau 2 years after ICI termination. The median ICI-free survival for the completion group and discontinuation group was not reached and 9.4 months, respectively (adjusted HR 0.28, p = 0.01). Estimated ICI-free survival rates in the completion and discontinuation groups were 80% vs. 38% at 1 year, 66% vs. 30% at 2 years, and 66% vs. 28% at 3 years.</p><p><strong>Conclusion: </strong>Patients who discontinued ICI therapy had poorer ICI-free survival than those who completed it. However, there was a notable population of patients with long-term ICI-free survival.</p>","PeriodicalId":23338,"journal":{"name":"Thoracic Cancer","volume":"16 11","pages":"e70090"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12130280/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/1759-7714.70090","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Immune checkpoint inhibitors (ICI)-containing therapy for advanced or recurrent non-small cell lung cancer (NSCLC) are not completed by some responders for reasons other than progressive disease (PD). The proportion of patients who discontinue ICI and the length of their treatment-free status are unclear.
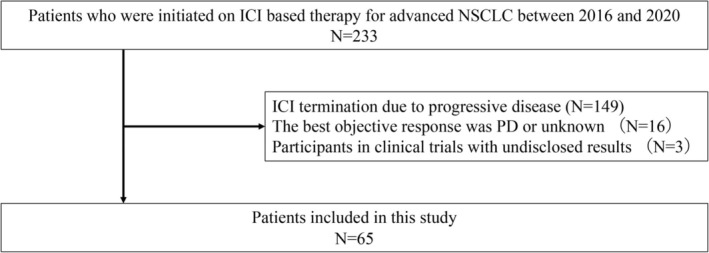
Methods: In this single-center retrospective study, we examined the medical records of 233 patients who initiated ICI-based therapy at our hospital between 2016 and 2020. We identified patients who completed treatment and discontinued it for reasons other than PD. The primary outcome was treatment-free survival, which we termed ICI-free survival.
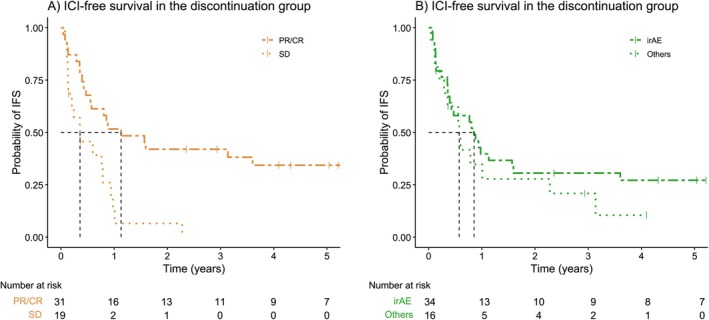
Results: Sixty-five patients were eligible for analysis. In the discontinuation group, the median duration of ICI was 3.9 months. Median progression-free survival, ICI-free survival, and overall survival in the entire population were 25.0, 11.5, and 78.3 months, respectively. The ICI-free survival rates at 1, 2, and 3 years were 48%, 38%, and 36%. The Kaplan-Meier curve of ICI-free survival almost reached a plateau 2 years after ICI termination. The median ICI-free survival for the completion group and discontinuation group was not reached and 9.4 months, respectively (adjusted HR 0.28, p = 0.01). Estimated ICI-free survival rates in the completion and discontinuation groups were 80% vs. 38% at 1 year, 66% vs. 30% at 2 years, and 66% vs. 28% at 3 years.
Conclusion: Patients who discontinued ICI therapy had poorer ICI-free survival than those who completed it. However, there was a notable population of patients with long-term ICI-free survival.
背景:含有免疫检查点抑制剂(ICI)的晚期或复发性非小细胞肺癌(NSCLC)治疗由于疾病进展(PD)以外的原因,一些应答者不能完成治疗。停止ICI的患者比例及其无治疗状态的持续时间尚不清楚。方法:在这项单中心回顾性研究中,我们检查了2016年至2020年在我院接受ici治疗的233例患者的病历。我们确定了完成治疗并因PD以外的原因停止治疗的患者。主要终点是无治疗生存期,我们称之为无ici生存期。结果:65例患者符合分析条件。在停药组,ICI的中位持续时间为3.9个月。整个人群的中位无进展生存期、无ici生存期和总生存期分别为25.0个月、11.5个月和78.3个月。1年、2年和3年无ici生存率分别为48%、38%和36%。无ICI生存的Kaplan-Meier曲线在ICI终止后2年几乎达到平台期。完成组和停药组的中位无ici生存期分别为未达到和9.4个月(调整后HR 0.28, p = 0.01)。完成组和停药组1年无ici生存率分别为80%对38%,66%对30%,3年66%对28%。结论:与完成ICI治疗的患者相比,停止ICI治疗的患者无ICI生存期较差。然而,有相当一部分患者的长期无ici生存。
期刊介绍:
Thoracic Cancer aims to facilitate international collaboration and exchange of comprehensive and cutting-edge information on basic, translational, and applied clinical research in lung cancer, esophageal cancer, mediastinal cancer, breast cancer and other thoracic malignancies. Prevention, treatment and research relevant to Asia-Pacific is a focus area, but submissions from all regions are welcomed. The editors encourage contributions relevant to prevention, general thoracic surgery, medical oncology, radiology, radiation medicine, pathology, basic cancer research, as well as epidemiological and translational studies in thoracic cancer. Thoracic Cancer is the official publication of the Chinese Society of Lung Cancer, International Chinese Society of Thoracic Surgery and is endorsed by the Korean Association for the Study of Lung Cancer and the Hong Kong Cancer Therapy Society.
The Journal publishes a range of article types including: Editorials, Invited Reviews, Mini Reviews, Original Articles, Clinical Guidelines, Technological Notes, Imaging in thoracic cancer, Meeting Reports, Case Reports, Letters to the Editor, Commentaries, and Brief Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


