GIANT: a prospective, multicenter, real-world study on the effectiveness, safety, and tolerability of atogepant in migraine patients with multiple therapeutic failures.
Piero Barbanti, Gabriella Egeo, Francesca Pistoia, Cinzia Aurilia, Paola Scatena, Steno Rinalduzzi, Silvia Strumia, Antonio Salerno, Fabio Frediani, Andrea Galli, Massimo Autunno, Laura Di Clemente, Maurizio Zucco, Maria Albanese, Francesco Bono, Pietrantonio Bruno, Laura Borrello, Stefano Messina, Alberto Doretti, Angelo Ranieri, Cecilia Camarda, Rosario Vecchio, Valeria Drago, Giulia Fiorentini, Carlo Tomino, Stefano Bonassi, Paola Torelli, Alice Mannocci
{"title":"GIANT: a prospective, multicenter, real-world study on the effectiveness, safety, and tolerability of atogepant in migraine patients with multiple therapeutic failures.","authors":"Piero Barbanti, Gabriella Egeo, Francesca Pistoia, Cinzia Aurilia, Paola Scatena, Steno Rinalduzzi, Silvia Strumia, Antonio Salerno, Fabio Frediani, Andrea Galli, Massimo Autunno, Laura Di Clemente, Maurizio Zucco, Maria Albanese, Francesco Bono, Pietrantonio Bruno, Laura Borrello, Stefano Messina, Alberto Doretti, Angelo Ranieri, Cecilia Camarda, Rosario Vecchio, Valeria Drago, Giulia Fiorentini, Carlo Tomino, Stefano Bonassi, Paola Torelli, Alice Mannocci","doi":"10.1186/s10194-025-02068-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atogepant, the first oral CGRP receptor antagonist approved for migraine prevention, has demonstrated efficacy and safety in randomized clinical trials (RCT). However, prospective real-world data are lacking.</p><p><strong>Objective: </strong>To explore the effectiveness, safety, and tolerability of atogepant 60 mg at week 12 in patients with high-frequency episodic (HFEM: 8-14 days/month) or chronic migraine (CM) with multiple therapeutic failures.</p><p><strong>Methods: </strong>This ongoing, multicenter (n = 16), prospective real-world study included consecutive adults with HFEM or CM who had failed ≥3 prior preventive treatments, according to AIFA criteria. Participants received atogepant 60 mg daily, with treatment planned for up to 12 months.</p><p><strong>Primary endpoint: </strong>change from baseline to week 12 in monthly migraine days (MMD) for HFEM and monthly headache days (MHD) for CM. Secondary endpoints: changes in monthly analgesic intake (MAI), pain intensity (NRS), disability (HIT-6, MIDAS), interictal burden (MIBS-4), treatment satisfaction (PGIC), responder rates (≥ 50%, ≥ 75%, 100%), and changes in migraine frequency during the first treatment week compared to the last pre-treatment week. Adverse events were monitored throughout.</p><p><strong>Results: </strong>A total of 183 patients were enrolled and 82 completed ≥ 12 weeks of follow-up. Of these, 41.5% had previously failed anti-CGRP mAbs. At week 12, significant reductions (p < 0.001) were observed in MMD (-6.0) and MHD (-11.2). Secondary outcomes also improved significantly (p < 0.001): MAI (-10.9), NRS (-2.7), HIT-6 (-13.2), MIDAS (-61.1), and MIBS-4 (-5.4). Responder rates were 65.9% (≥ 50%), 36.6% (≥ 75%), and 6.1% (100%). PGIC documented high satisfaction (much/very much improved: 70.7%). A significant decrease (p < 0.001) in migraine frequency was already evident by week 1 (overall: - 2.5 days, HFEM: - 1.5, CM: - 3.1). In the mAb-failure subgroup, ≥ 50% and ≥ 75% response rates were 52.9% and 23.5%, with significant improvements in all primary and secondary endpoints (p < 0.001). Adverse events occurred in 5.5% of patients, and 1.6% discontinued treatment.</p><p><strong>Conclusion: </strong>The GIANT study provides real-world evidence of atogepant's effectiveness, safety, and tolerability in patients with HFEM and CM with multiple therapeutic failures and comorbidities. It extends RCT data by showing rapid onset of action, meaningful reductions in pain intensity and interictal disability, high patient satisfaction, and effectiveness even in patients with anti-CGRP mAb failures.</p>","PeriodicalId":16013,"journal":{"name":"Journal of Headache and Pain","volume":"26 1","pages":"122"},"PeriodicalIF":7.9000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12090485/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Headache and Pain","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s10194-025-02068-2","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Atogepant, the first oral CGRP receptor antagonist approved for migraine prevention, has demonstrated efficacy and safety in randomized clinical trials (RCT). However, prospective real-world data are lacking.
Objective: To explore the effectiveness, safety, and tolerability of atogepant 60 mg at week 12 in patients with high-frequency episodic (HFEM: 8-14 days/month) or chronic migraine (CM) with multiple therapeutic failures.
Methods: This ongoing, multicenter (n = 16), prospective real-world study included consecutive adults with HFEM or CM who had failed ≥3 prior preventive treatments, according to AIFA criteria. Participants received atogepant 60 mg daily, with treatment planned for up to 12 months.
Primary endpoint: change from baseline to week 12 in monthly migraine days (MMD) for HFEM and monthly headache days (MHD) for CM. Secondary endpoints: changes in monthly analgesic intake (MAI), pain intensity (NRS), disability (HIT-6, MIDAS), interictal burden (MIBS-4), treatment satisfaction (PGIC), responder rates (≥ 50%, ≥ 75%, 100%), and changes in migraine frequency during the first treatment week compared to the last pre-treatment week. Adverse events were monitored throughout.
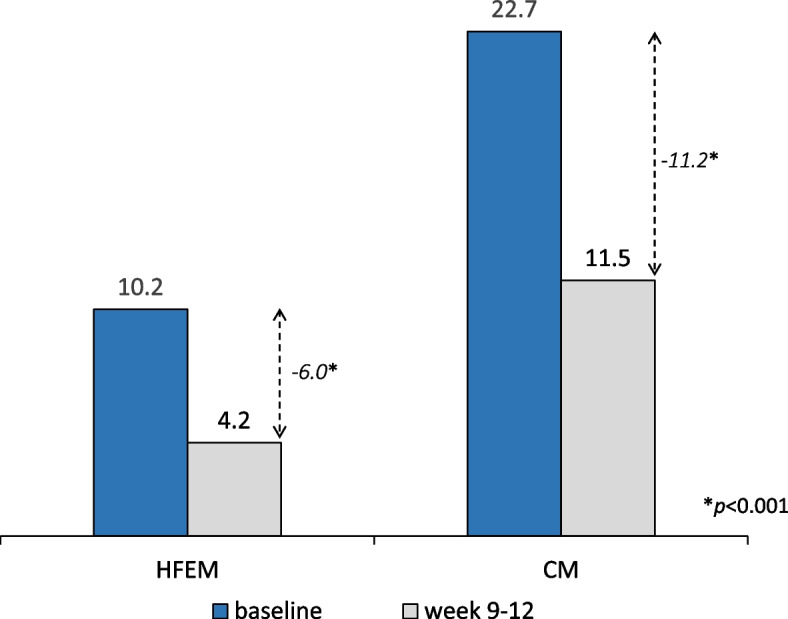
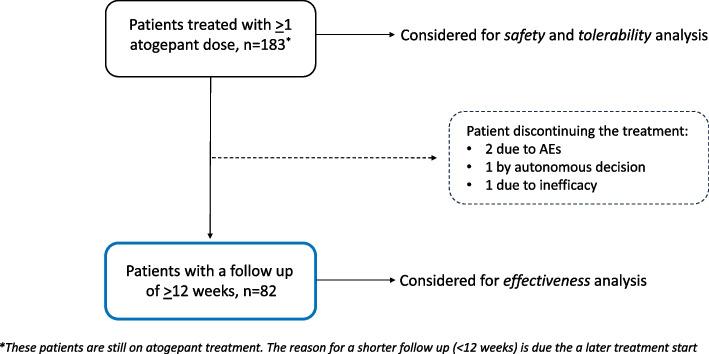
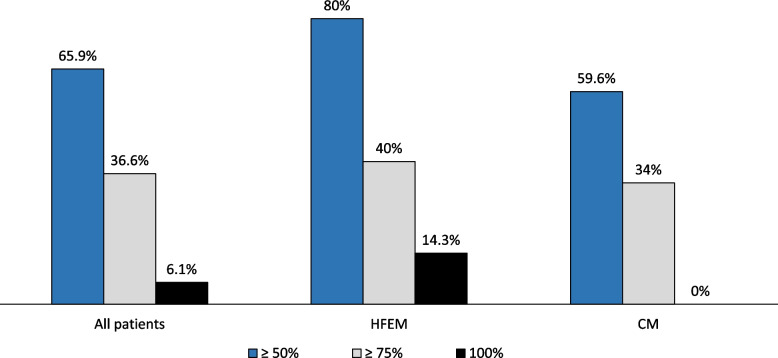
Results: A total of 183 patients were enrolled and 82 completed ≥ 12 weeks of follow-up. Of these, 41.5% had previously failed anti-CGRP mAbs. At week 12, significant reductions (p < 0.001) were observed in MMD (-6.0) and MHD (-11.2). Secondary outcomes also improved significantly (p < 0.001): MAI (-10.9), NRS (-2.7), HIT-6 (-13.2), MIDAS (-61.1), and MIBS-4 (-5.4). Responder rates were 65.9% (≥ 50%), 36.6% (≥ 75%), and 6.1% (100%). PGIC documented high satisfaction (much/very much improved: 70.7%). A significant decrease (p < 0.001) in migraine frequency was already evident by week 1 (overall: - 2.5 days, HFEM: - 1.5, CM: - 3.1). In the mAb-failure subgroup, ≥ 50% and ≥ 75% response rates were 52.9% and 23.5%, with significant improvements in all primary and secondary endpoints (p < 0.001). Adverse events occurred in 5.5% of patients, and 1.6% discontinued treatment.
Conclusion: The GIANT study provides real-world evidence of atogepant's effectiveness, safety, and tolerability in patients with HFEM and CM with multiple therapeutic failures and comorbidities. It extends RCT data by showing rapid onset of action, meaningful reductions in pain intensity and interictal disability, high patient satisfaction, and effectiveness even in patients with anti-CGRP mAb failures.
期刊介绍:
The Journal of Headache and Pain, a peer-reviewed open-access journal published under the BMC brand, a part of Springer Nature, is dedicated to researchers engaged in all facets of headache and related pain syndromes. It encompasses epidemiology, public health, basic science, translational medicine, clinical trials, and real-world data.
With a multidisciplinary approach, The Journal of Headache and Pain addresses headache medicine and related pain syndromes across all medical disciplines. It particularly encourages submissions in clinical, translational, and basic science fields, focusing on pain management, genetics, neurology, and internal medicine. The journal publishes research articles, reviews, letters to the Editor, as well as consensus articles and guidelines, aimed at promoting best practices in managing patients with headaches and related pain.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


