The Cost-Effectiveness of Early Active Mobilization During Mechanical Ventilation in the ICU: An Economic Evaluation Alongside the Treatment of Mechanically Ventilated Adults With Early Activity and Mobilization (TEAM) Trial.
Alisa M Higgins, Yong Yi Lee, Michael Bailey, Rinaldo Bellomo, Kathy Brickell, Tessa Broadley, Heidi Buhr, Belinda J Gabbe, Doug W Gould, Meg Harrold, Sally Hurford, Theodore J Iwashyna, Ary Serpa Neto, Alistair D Nichol, Jeffrey J Presneill, Stefan J Schaller, Janani Sivasuthan, Claire J Tipping, Steven Webb, Paul J Young, Carol L Hodgson
{"title":"The Cost-Effectiveness of Early Active Mobilization During Mechanical Ventilation in the ICU: An Economic Evaluation Alongside the Treatment of Mechanically Ventilated Adults With Early Activity and Mobilization (TEAM) Trial.","authors":"Alisa M Higgins, Yong Yi Lee, Michael Bailey, Rinaldo Bellomo, Kathy Brickell, Tessa Broadley, Heidi Buhr, Belinda J Gabbe, Doug W Gould, Meg Harrold, Sally Hurford, Theodore J Iwashyna, Ary Serpa Neto, Alistair D Nichol, Jeffrey J Presneill, Stefan J Schaller, Janani Sivasuthan, Claire J Tipping, Steven Webb, Paul J Young, Carol L Hodgson","doi":"10.1097/CCM.0000000000006715","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Early mobilization is recommended by the Society of Critical Care Medicine ICU Liberation Bundle. The Treatment of Mechanically Ventilated Adults With Early Activity and Mobilization (TEAM) randomized controlled trial (RCT) compared early active mobilization to usual care mobilization and found no difference in the primary outcome of days alive and out of hospital to day 180; however, it did find an increase in adverse events in the intervention group. To date, no RCT of early mobilization has reported costs or cost-effectiveness. We aimed to determine the cost-effectiveness of early active mobilization from the perspective of the healthcare sector.</p><p><strong>Design: </strong>We conducted a prospective, within-trial cost-effectiveness analysis alongside the TEAM study.</p><p><strong>Setting: </strong>Forty-nine ICUs in six countries (Australia, New Zealand, United Kingdom, Ireland, Germany, and Brazil).</p><p><strong>Patients: </strong>The cost-effectiveness analysis included 733 adult ICU patients who were undergoing invasive mechanical ventilation and enrolled in the TEAM study.</p><p><strong>Interventions: </strong>Early active mobilization or usual care mobilization.</p><p><strong>Measurements and main results: </strong>A significantly higher number of hours were spent by staff in delivering high-dose early active mobilization vs. usual care mobilization; however, incremental costs were not significantly different between the groups ($1,823; 95% CI, -$10,552 to $12,027). EuroQoL-5D 5-level utility scores at 6 months were not significantly different between the groups (0.532 [ se , 0.021] vs. 0.548 [ se , 0.021]; p = 0.585). The probability of early active mobilization being cost-effective is less than 50%, even at a willingness-to-pay threshold of $200,000/quality-adjusted life year (QALY). Sensitivity analyses incorporating meta-analysis data indicated that early active mobilization may be cost-saving; however, this involves the occurrence of lower QALY gains when compared with usual care mobilization.</p><p><strong>Conclusions: </strong>Our trial-based analysis found no evidence that higher-dose early active mobilization is a cost-effective intervention compared with usual care mobilization for mechanically ventilated adult ICU patients; however, results from sensitivity analyses provided some evidence that it may be cost saving if one is willing to accept poorer outcomes. Further research is necessary to determine whether there are scenarios in which early active mobilization provides value for money.</p>","PeriodicalId":10765,"journal":{"name":"Critical Care Medicine","volume":" ","pages":"e1725-e1735"},"PeriodicalIF":6.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393053/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/CCM.0000000000006715","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Early mobilization is recommended by the Society of Critical Care Medicine ICU Liberation Bundle. The Treatment of Mechanically Ventilated Adults With Early Activity and Mobilization (TEAM) randomized controlled trial (RCT) compared early active mobilization to usual care mobilization and found no difference in the primary outcome of days alive and out of hospital to day 180; however, it did find an increase in adverse events in the intervention group. To date, no RCT of early mobilization has reported costs or cost-effectiveness. We aimed to determine the cost-effectiveness of early active mobilization from the perspective of the healthcare sector.
Design: We conducted a prospective, within-trial cost-effectiveness analysis alongside the TEAM study.
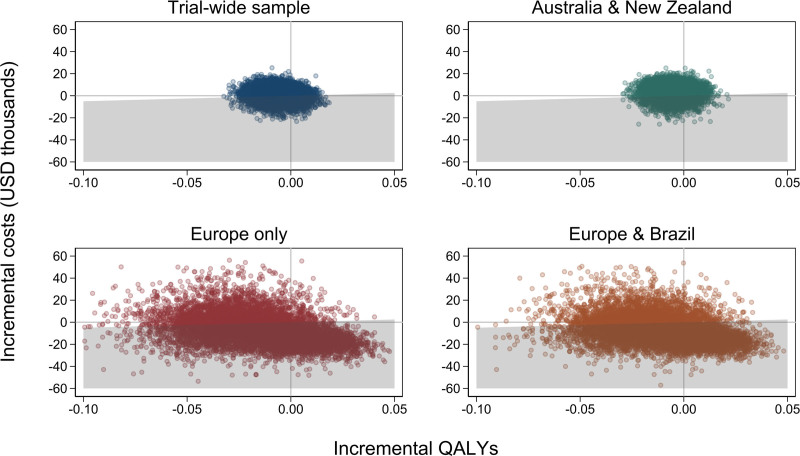
Setting: Forty-nine ICUs in six countries (Australia, New Zealand, United Kingdom, Ireland, Germany, and Brazil).
Patients: The cost-effectiveness analysis included 733 adult ICU patients who were undergoing invasive mechanical ventilation and enrolled in the TEAM study.
Interventions: Early active mobilization or usual care mobilization.
Measurements and main results: A significantly higher number of hours were spent by staff in delivering high-dose early active mobilization vs. usual care mobilization; however, incremental costs were not significantly different between the groups ($1,823; 95% CI, -$10,552 to $12,027). EuroQoL-5D 5-level utility scores at 6 months were not significantly different between the groups (0.532 [ se , 0.021] vs. 0.548 [ se , 0.021]; p = 0.585). The probability of early active mobilization being cost-effective is less than 50%, even at a willingness-to-pay threshold of $200,000/quality-adjusted life year (QALY). Sensitivity analyses incorporating meta-analysis data indicated that early active mobilization may be cost-saving; however, this involves the occurrence of lower QALY gains when compared with usual care mobilization.
Conclusions: Our trial-based analysis found no evidence that higher-dose early active mobilization is a cost-effective intervention compared with usual care mobilization for mechanically ventilated adult ICU patients; however, results from sensitivity analyses provided some evidence that it may be cost saving if one is willing to accept poorer outcomes. Further research is necessary to determine whether there are scenarios in which early active mobilization provides value for money.
期刊介绍:
Critical Care Medicine is the premier peer-reviewed, scientific publication in critical care medicine. Directed to those specialists who treat patients in the ICU and CCU, including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals, Critical Care Medicine covers all aspects of acute and emergency care for the critically ill or injured patient.
Each issue presents critical care practitioners with clinical breakthroughs that lead to better patient care, the latest news on promising research, and advances in equipment and techniques.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


